

Do poor people in the poorer states pay more for healthcare in India?
- PMID: 31362727
- PMCID: PMC6668144
- DOI: 10.1186/s12889-019-7342-8
Do poor people in the poorer states pay more for healthcare in India?
Abstract
Background: Rising health spending is associated with high out-of-pocket expenditure (OOPE), catastrophic health spending (CHS), increasing poverty, and impoverishment. Though studies have examined poverty and impoverishment effect of health spending in India, there is limited research on the regional patterns of health spending by type of health centers. This paper tests the hypothesis that the poor people from the poorer states of India pay significantly more for hospitalization in public health centers than those in the richer states of India.
Methods: Data from the Social Consumption of Health Survey (71st round, 2014), carried out by the National Sample Survey (NSS) is used in the analyses. Descriptive statistics, log-linear regression model and tobit model were used to examine the determinants and variations in health spending.
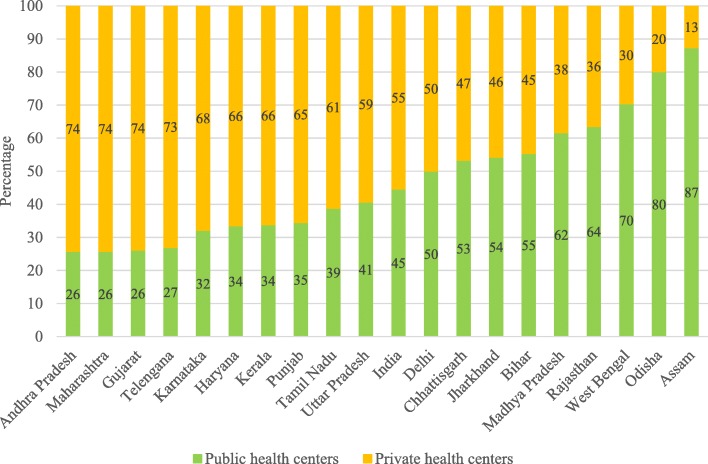
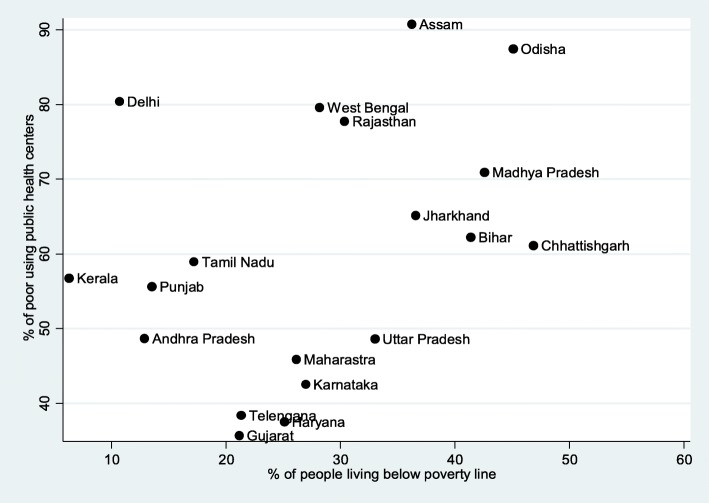
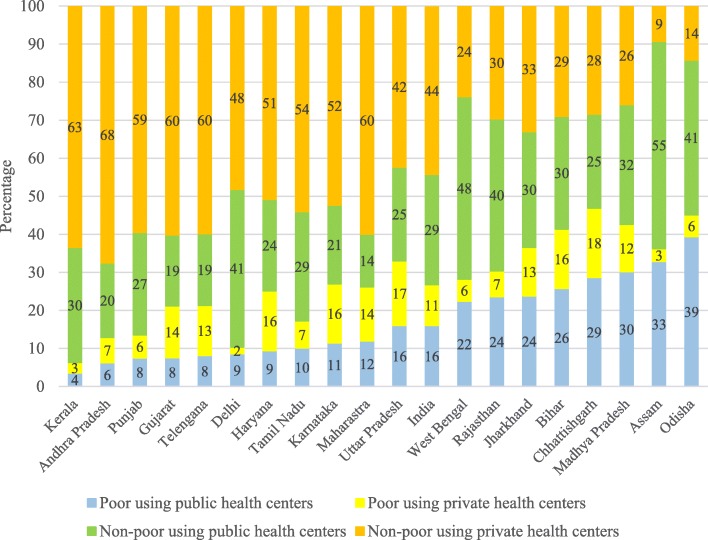
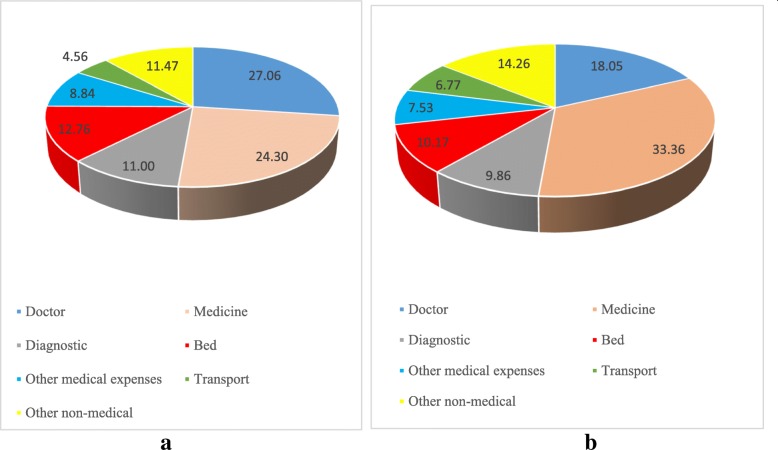
Results: Inter-state variations in the utilization of public health services and the OOPE on hospitalization are high in India. States with high levels of poverty make higher use of the public health centers and yet incur high OOPE. In 2014, the mean OOPE per episode of hospitalization in public health centers in India was ₹5688 and ₹4264 for the economically poor households. It was lowest in the economically developed state of Tamil Nadu and highest in the economically poorer state of Bihar. The OOPE per episode of hospitalization in public health centers among the poor in the poorer states was at least twice that in Tamil Nadu. Among the poor using public health centers, the share of direct cost account 24% in Tamil Nadu compared to over 80% in Bihar, Odisha and other poorer states. Adjusting for socio-economic correlates, the cost of hospitalization per episode (CHPE) among the poor using public health centers was 51% lower than for the non-poor using private health centers in India.
Conclusion: The poor people in the poorer states in India pay significantly more to avail hospitalization in public health centers than those in the developed states. Provision of free medicines, surgery and free diagnostic tests in public health centers may reduce the high OOPE and medical poverty in India.
Keywords: Financial protection; Hospitalization; India; Out-of-pocket expenditure; Poverty; Public health.
Conflict of interest statement
The authors declare that they have no competing interests..
Figures
References
-
- WHO. World health statistics: monitoring health for the SDGs. 2018. [http://apps.who.int/iris/bitstream/handle/10665/272596/9789241565585-eng...]. Accessed 20 Jan 2019.
-
- O’Donnell O, van Doorslaer E, Rannan-Eliya RP, Somanathan A, Adhikari SR, Harbianto D, et al. The incidence of public spending on healthcare: comparative evidence from Asia. World Bank Econ Rev. 2007;21(1):93–123. doi: 10.1093/wber/lhl009. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
