

Tranexamic acid for acute gastrointestinal bleeding (the HALT-IT trial): statistical analysis plan for an international, randomised, double-blind, placebo-controlled trial
- PMID: 31362765
- PMCID: PMC6668177
- DOI: 10.1186/s13063-019-3561-7
Tranexamic acid for acute gastrointestinal bleeding (the HALT-IT trial): statistical analysis plan for an international, randomised, double-blind, placebo-controlled trial
Abstract
Background: Acute gastrointestinal (GI) bleeding is an important cause of mortality worldwide. Bleeding can occur from the upper or lower GI tract, with upper GI bleeding accounting for most cases. The main causes include peptic ulcer/erosive mucosal disease, oesophageal varices and malignancy. The case fatality rate is around 10% for upper GI bleeding and 3% for lower GI bleeding. Rebleeding affects 5-40% of patients and is associated with a four-fold increased risk of death. Tranexamic acid (TXA) decreases bleeding and the need for blood transfusion in surgery and reduces death due to bleeding in patients with trauma and postpartum haemorrhage. It reduces bleeding by inhibiting the breakdown of fibrin clots by plasmin. Due to the methodological weaknesses and small size of the existing trials, the effectiveness and safety of TXA in GI bleeding is uncertain. The Haemorrhage ALleviation with Tranexamic acid - Intestinal system (HALT-IT) trial aims to provide reliable evidence about the effects of TXA in acute upper and lower GI bleeding.
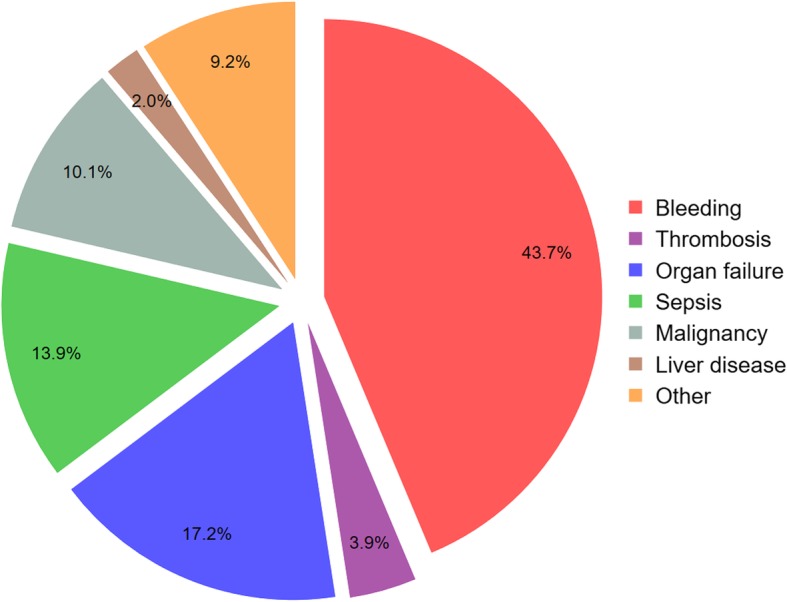
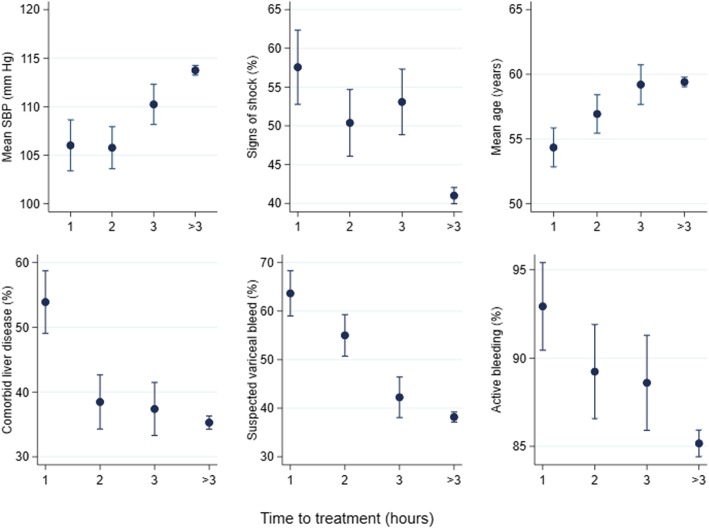
Methods: The HALT-IT trial is an international, randomised, double-blind, placebo-controlled trial of tranexamic acid in 12,000 adults (increased from 8000) with acute upper or lower GI bleeding. Eligible patients are randomly allocated to receive TXA (1-g loading dose followed by 3-g maintenance dose over 24 h) or matching placebo. The main analysis will compare those randomised to TXA with those randomised to placebo on an intention-to-treat basis, presenting the results as effect estimates (relative risks) and confidence intervals. The primary outcome is death due to bleeding within 5 days of randomisation and secondary outcomes are: rebleeding; all-cause and cause-specific mortality; thromboembolic events; complications; endoscopic, radiological and surgical interventions; blood transfusion requirements; disability (defined by a measure of patient's self-care capacity); and number of days spent in intensive care or high-dependency units. Subgroup analyses for the primary outcome will consider time to treatment, location of bleeding, cause of bleed and clinical Rockall score.
Discussion: We present the statistical analysis of the HALT-IT trial. This plan was published before the treatment allocation was unblinded.
Trial registration: Current Controlled Trials, ID: ISRCTN11225767. Registered on 3 July 2012; Clinicaltrials.gov, ID: NCT01658124. Registered on 26 July 2012.
Keywords: Clinical trial; Gastrointestinal haemorrhage; Statistical analysis; Tranexamic acid.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Theocharis George J., Thomopoulos Konstantinos C., Sakellaropoulos George, Katsakoulis Evangelos, Nikolopoulou Vassiliki. Changing Trends in the Epidemiology and Clinical Outcome of Acute Upper Gastrointestinal Bleeding in a Defined Geographical Area in Greece. Journal of Clinical Gastroenterology. 2008;42(2):128–133. doi: 10.1097/01.mcg.0000248004.73075.ad. - DOI - PubMed
-
- van Leerdam M, Vreeburg E, Rauws EA, Geraedts AA, Tijssen JG, Reitsma J, et al. Acute upper GI bleeding: did anything change?: time trend analysis of incidence and outcome of acute upper GI bleeding between 1993/1994 and 2000. Am J Gastroenterol. 2003;98:1494–1499. doi: 10.1111/j.1572-0241.2003.07517.x. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
