

Readiness of public health facilities to provide quality maternal and newborn care across the state of Bihar, India: a cross-sectional study of district hospitals and primary health centres
- PMID: 31362965
- PMCID: PMC6678016
- DOI: 10.1136/bmjopen-2018-028370
Readiness of public health facilities to provide quality maternal and newborn care across the state of Bihar, India: a cross-sectional study of district hospitals and primary health centres
Erratum in
-
Correction: Readiness of public health facilities to provide quality maternal and newborn care across the state of Bihar, India: a cross-sectional study of district hospitals and primary health centres.BMJ Open. 2019 Aug 30;9(8):e028370corr1. doi: 10.1136/bmjopen-2018-028370corr1. BMJ Open. 2019. PMID: 31471445 Free PMC article. No abstract available.
Abstract
Introduction: Poor access to quality healthcare is one of the most important reasons of high maternal and neonatal mortality in India, particularly in poorer states like Bihar. India has implemented initiatives to promote institutional maternal deliveries. It is important to ensure that health facilities are adequately equipped and staffed to provide quality care for mothers and newborns.
Methods: We conducted a cross-sectional study of 190 primary health centres (PHCs) and 36 district hospitals (DHs) across all districts in Bihar to assess the readiness of facilities to provide quality maternal and neonatal care. Infrastructure, equipment and supplies and staffing were assessed using the WHO service availability and readiness assessment and Indian public health standard guidelines. Additionally, we used household survey data to assess the quality of care reported by mothers delivering at study facilities.
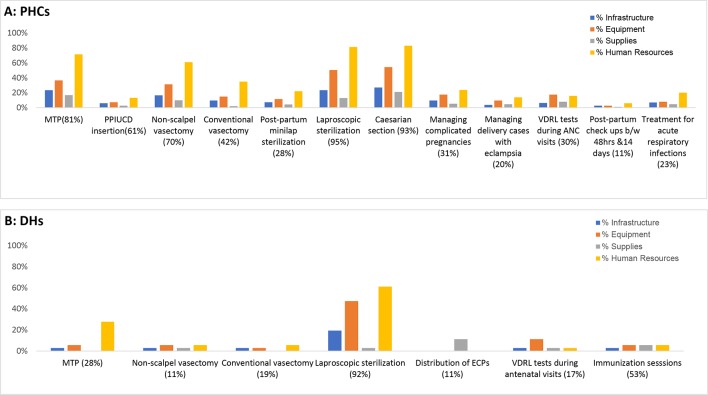
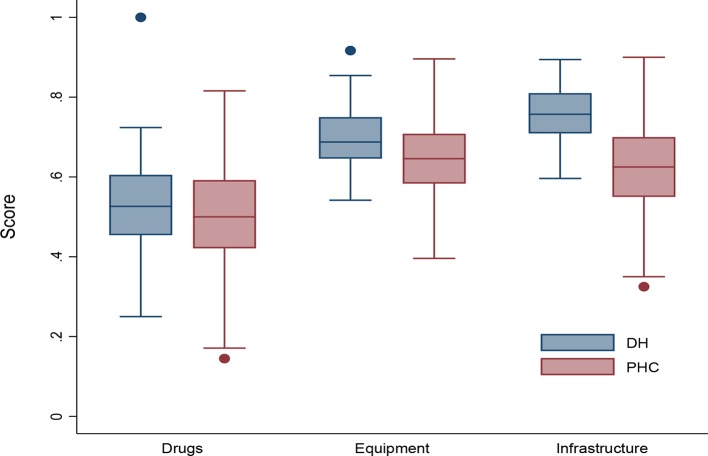
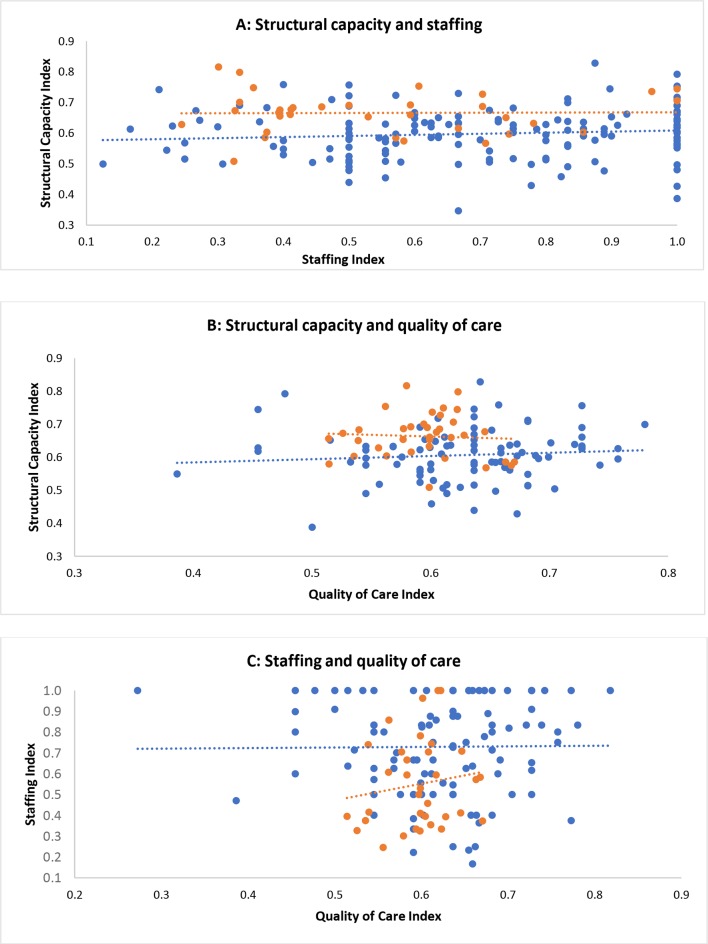
Results: PHCs and DHs were found to have 61% and 67% of the mandated structural components to provide maternal and neonatal care, on average, respectively. DHs were, on average, slightly better equipped in terms of infrastructure, equipment and supplies by comparison to PHCs. DHs were found to be inadequately prepared to provide neonatal care. Lack of recommended handwashing stations and bins at both DHs and PHCs suggested low levels of hygiene. Only half of the essential drugs were available in both DHs and PHCs. While no association was revealed between structural capacity and patient-reported quality of care, adequacy of staffing was positively associated with the quality of care in DHs.
Conclusion: Examining all DHs and a representative sample of PHCs in Bihar, this study revealed the gaps in structural components that need to be filled to provide quality care to mothers and newborns. Access to quality care is essential if progress in reducing maternal and neonatal mortality is to be achieved in this high-burden state.
Keywords: health economics; health policy; quality in health care.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- WHO, UNICEF, UNFPA, World Bank Group and UNPD. Maternal mortality in 1990-2015. 2015.
-
- Wang H, Bhutta ZA, Coates MM, et al. Global, regional, national, and selected subnational levels of stillbirths, neonatal, infant, and under-5 mortality, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. The Lancet 2016;388:1725–74. 10.1016/S0140-6736(16)31575-6 - DOI - PMC - PubMed
-
- Sustainable Development Knowledge Platform.
-
- Government of India Planning Commission. Press note on poverty estimates, 2011-12: Press Information Bureau, 2013.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources