

Mice Fed an Obesogenic Western Diet, Administered Antibiotics, and Subjected to a Sterile Surgical Procedure Develop Lethal Septicemia with Multidrug-Resistant Pathobionts
- PMID: 31363025
- PMCID: PMC6667615
- DOI: 10.1128/mBio.00903-19
Mice Fed an Obesogenic Western Diet, Administered Antibiotics, and Subjected to a Sterile Surgical Procedure Develop Lethal Septicemia with Multidrug-Resistant Pathobionts
Abstract
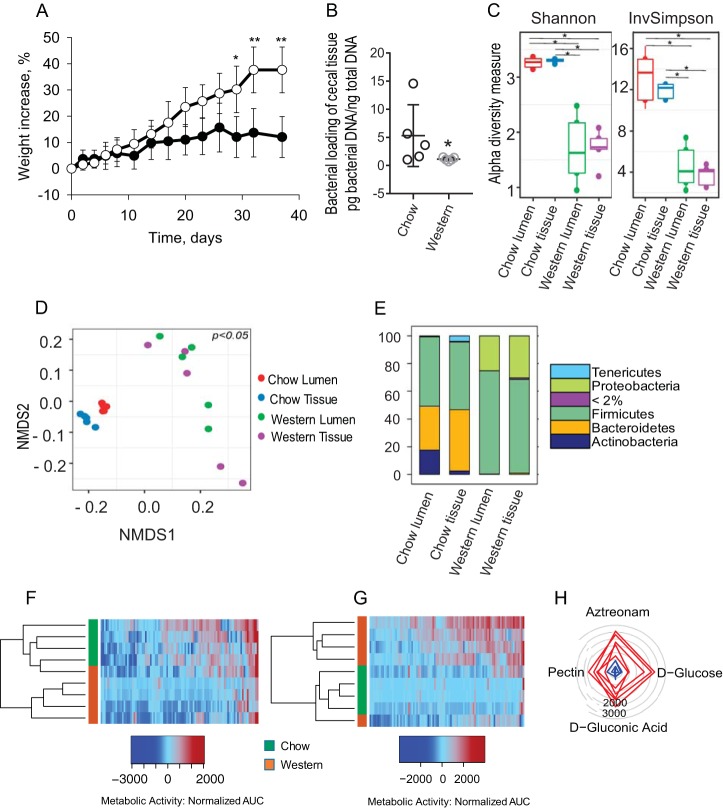
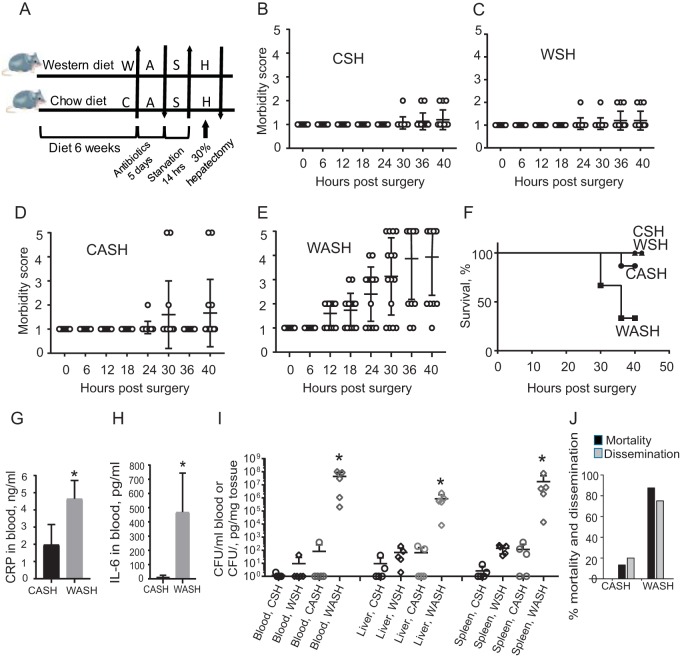
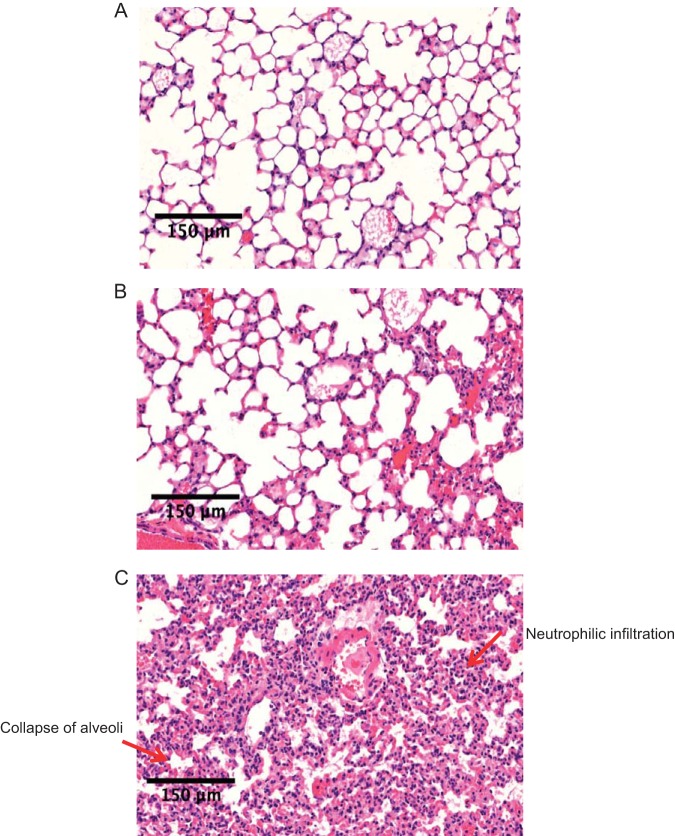
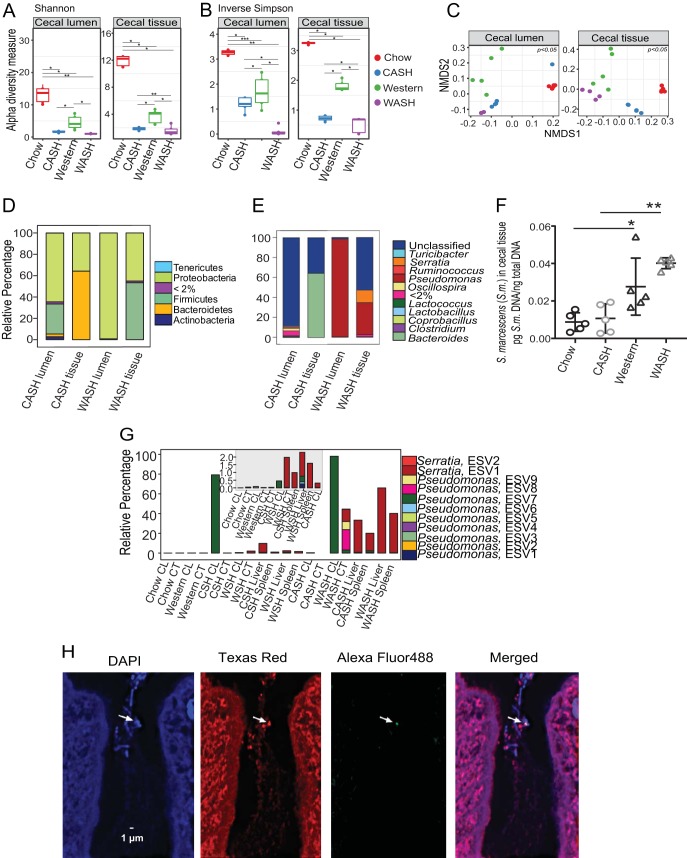
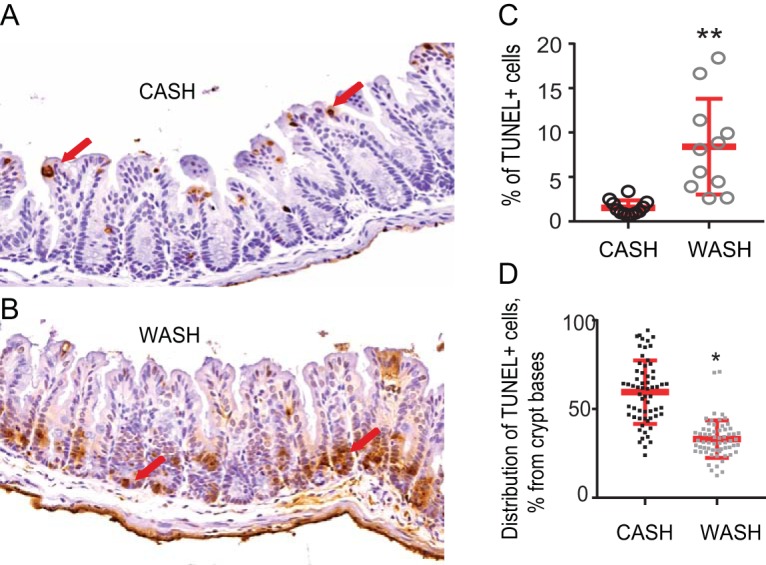
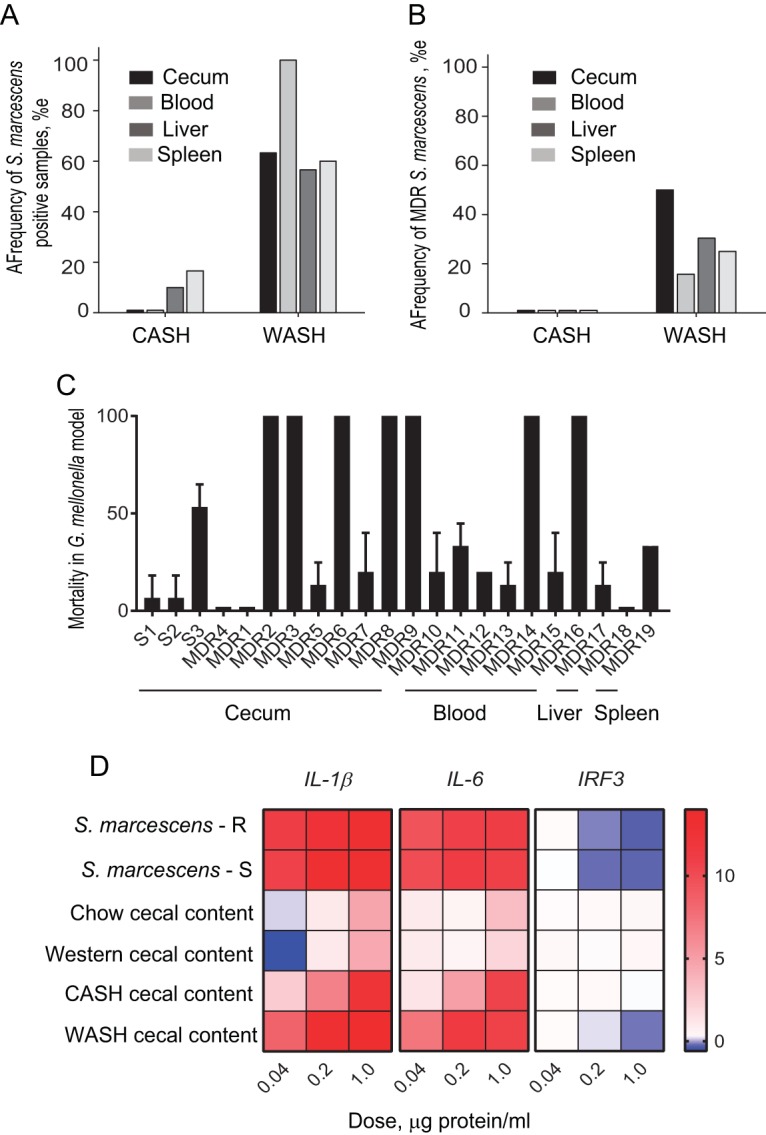
Despite antibiotics and sterile technique, postoperative infections remain a real and present danger to patients. Recent estimates suggest that 50% of the pathogens associated with postoperative infections have become resistant to the standard antibiotics used for prophylaxis. Risk factors identified in such cases include obesity and antibiotic exposure. To study the combined effect of obesity and antibiotic exposure on postoperative infection, mice were allowed to gain weight on an obesogenic Western-type diet (WD), administered antibiotics and then subjected to an otherwise recoverable sterile surgical injury (30% hepatectomy). The feeding of a WD alone resulted in a major imbalance of the cecal microbiota characterized by a decrease in diversity, loss of Bacteroidetes, a bloom in Proteobacteria, and the emergence of antibiotic-resistant organisms among the cecal microbiota. When WD-fed mice were administered antibiotics and subjected to 30% liver resection, lethal sepsis, characterized by multiple-organ damage, developed. Notable was the emergence and systemic dissemination of multidrug-resistant (MDR) pathobionts, including carbapenem-resistant, extended-spectrum β-lactamase-producing Serratia marcescens, which expressed a virulent and immunosuppressive phenotype. Analysis of the distribution of exact sequence variants belonging to the genus Serratia suggested that these strains originated from the cecal mucosa. No mortality or MDR pathogens were observed in identically treated mice fed a standard chow diet. Taken together, these results suggest that consumption of a Western diet and exposure to certain antibiotics may predispose to life-threating postoperative infection associated with MDR organisms present among the gut microbiota.IMPORTANCE Obesity remains a prevalent and independent risk factor for life-threatening infection following major surgery. Here, we demonstrate that when mice are fed an obesogenic Western diet (WD), they become susceptible to lethal sepsis with multiple organ damage after exposure to antibiotics and an otherwise-recoverable surgical injury. Analysis of the gut microbiota in this model demonstrates that WD alone leads to loss of Bacteroidetes, a bloom of Proteobacteria, and evidence of antibiotic resistance development even before antibiotics are administered. After antibiotics and surgery, lethal sepsis with organ damage developed in in mice fed a WD with the appearance of multidrug-resistant pathogens in the liver, spleen, and blood. The importance of these findings lies in exposing how the selective pressures of diet, antibiotic exposure, and surgical injury can converge on the microbiome, resulting in lethal sepsis and organ damage without the introduction of an exogenous pathogen.
Keywords: Western diet; gut microbiome; gut-derived sepsis; pathobionts; surgery.
Copyright © 2019 Hyoju et al.
Figures
Comment in
-
Live and Diet by Your Gut Microbiota.mBio. 2019 Oct 8;10(5):e02335-19. doi: 10.1128/mBio.02335-19. mBio. 2019. PMID: 31594820 Free PMC article.
References
-
- Călina D, Docea AO, Rosu L, Zlatian O, Rosu AF, Anghelina F, Rogoveanu O, Arsene AL, Nicolae AC, Drăgoi CM, Tsiaoussis J, Tsatsakis AM, Spandidos DA, Drakoulis N, Gofita E. 2017. Antimicrobial resistance development following surgical site infections. Mol Med Rep 15:681–688. doi: 10.3892/mmr.2016.6034. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
