

SONOELASTOGRAPHIC FEATURES OF HIGH-RISK BREAST LESIONS AND DUCTAL CARCINOMA IN SITU - A PILOT STUDY
- PMID: 31363320
- PMCID: PMC6629205
- DOI: 10.20471/acc.2019.58.01.02
SONOELASTOGRAPHIC FEATURES OF HIGH-RISK BREAST LESIONS AND DUCTAL CARCINOMA IN SITU - A PILOT STUDY
Abstract
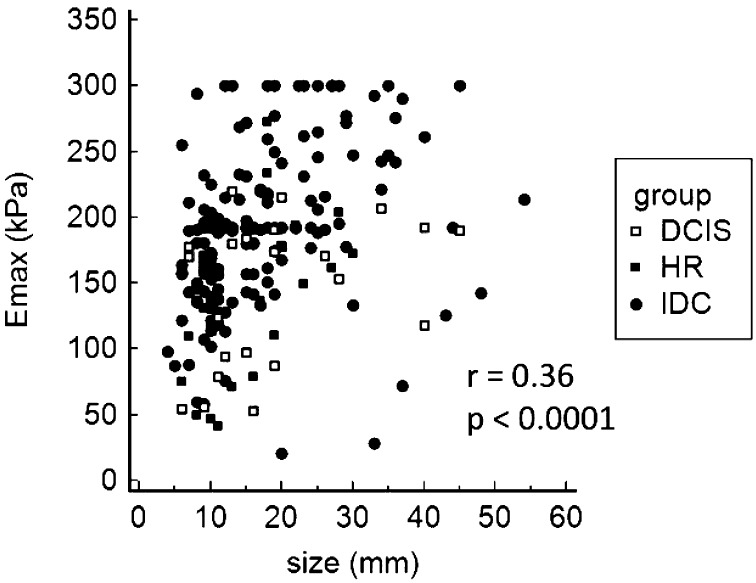
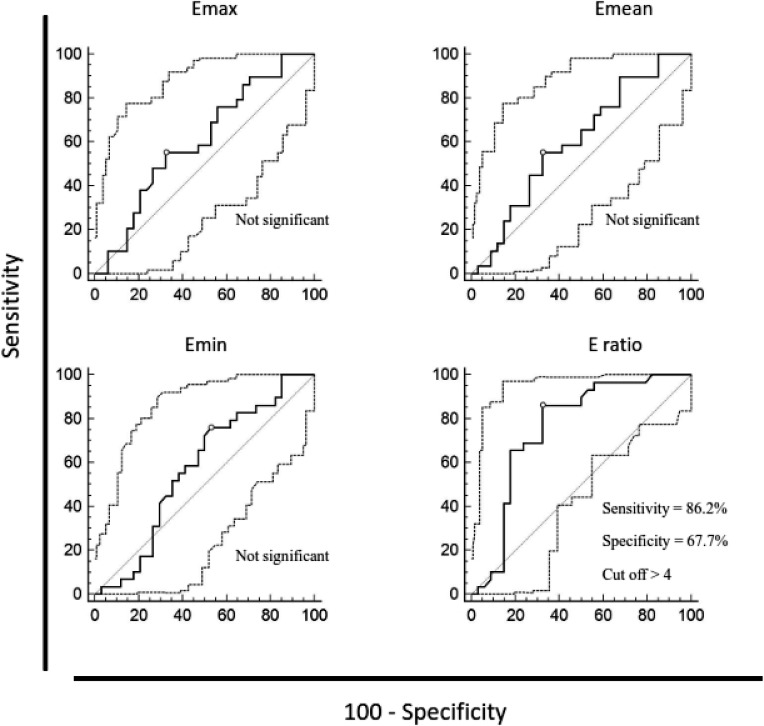
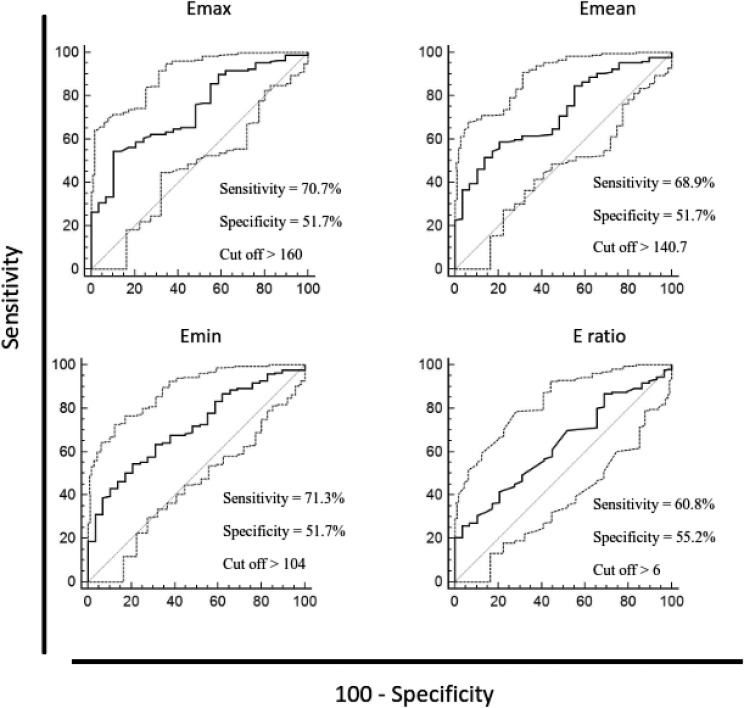
The aim of this study was to evaluate the quantitative sonoelastographic values recorded on shear-wave sonoelastography (SWE) of high-risk breast lesions and ductal carcinoma in situ (DCIS). We retrospectively analyzed histopathologic and SWE data (quantitative maximum, minimum and mean stiffness, lesion-to-fat ratio (E-ratio), lesion size) of 228 women referred to our Department for core needle breast biopsy during a four-year period. Among 230 lesions, histopathologic findings showed 34 high-risk breast lesions and 29 DCIS, which were compared with 167 ductal invasive carcinomas. High-risk lesions had lower values of all sonoelastographic features than ductal in situ and invasive carcinoma, however, only E-ratio showed a statistically significant difference in comparison to DCIS (3.7 vs. 6, p<0.001). All sonoelastographic features showed significant difference between in situ and invasive carcinoma. There was a significant correlation between lesion size and stiffness (r=0.36; p<0.001). Stiffness measured by SWE is an effective predictor of the histopathologic severity of sonographically detectable breast lesions. Elasticity values of high-risk lesions are significantly lower than those of malignant lesions. Furthermore, we showed that along with the sonographic appearance, which in most cases shows typical microcalcifications, DCIS had significantly different elasticity parameters than invasive carcinoma.
Keywords: Breast neoplasms – classification; Breast neoplasms – diagnostic imaging; Carcinoma, intraductal; Elastic modulus; Elasticity imaging techniques; Sensitivity and specificity; Shear-wave elastography (SWE); Ultrasonography, mammary.
Figures
References
-
- Croatian Institute for Public Health, Croatian National Cancer Registry. Bulletin no.38: Cancer incidence in Croatia 2013.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical