

ACUTE PHYSIOLOGY AND CHRONIC HEALTH EVALUATION (APACHE) II SCORE - THE CLINICAL PREDICTOR IN NEUROSURGICAL INTENSIVE CARE UNIT
- PMID: 31363325
- PMCID: PMC6629196
- DOI: 10.20471/acc.2019.58.01.07
ACUTE PHYSIOLOGY AND CHRONIC HEALTH EVALUATION (APACHE) II SCORE - THE CLINICAL PREDICTOR IN NEUROSURGICAL INTENSIVE CARE UNIT
Abstract
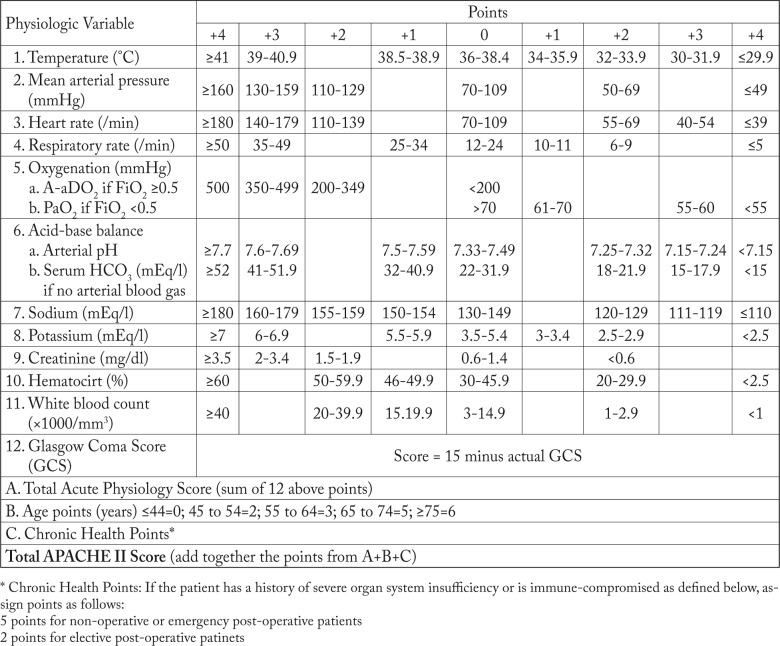
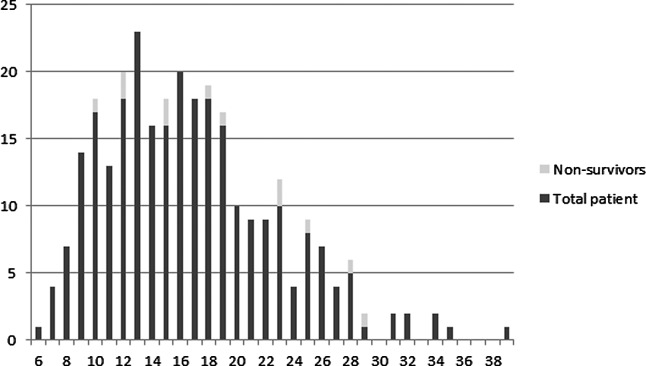
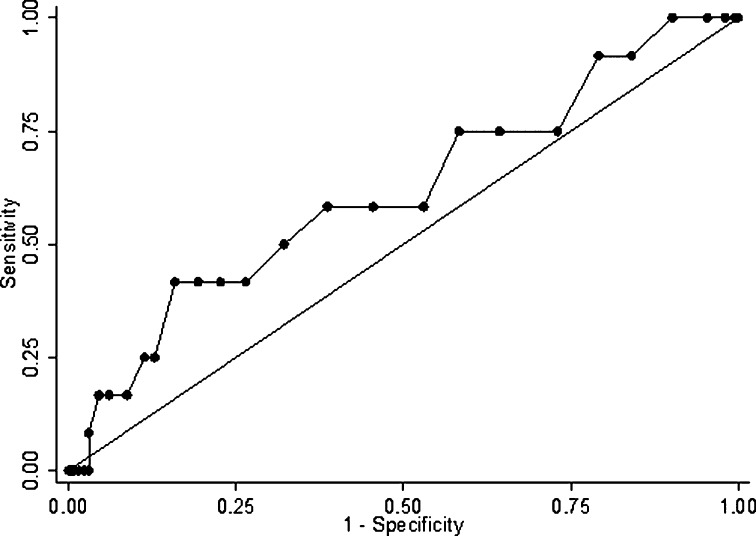
The APACHE II scoring system is approved for its benchmarking and mortality predictions, but there are only a few articles published to demonstrate it in neurosurgical patients. Therefore, this study was performed to acknowledge this score and its predictive performance to hospital mortality in a tertiary referral neurosurgical intensive care unit (ICU). All patients admitted to the Neurosurgical ICU from February 1 to July 31, 2011 were recruited. The parameters indicated in APACHE II score were collected. The adjusted predicted risk of death was calculated and compared with the death rate observed. Descriptive statistics including the receiver operating characteristic curve (ROC) was performed. The results showed that 276 patients were admitted during the mentioned period. The APACHE II score was 16.56 (95% CI, 15.84-17.29) and 19.08 (95% CI, 15.40-22.76) in survivors and non-survivors, while the adjusted predicted death rates were 13.39% (95% CI, 11.83-14.95) and 17.49% (95% CI, 9.81-25.17), respectively. The observed mortality was only 4.35%. The area under the ROC of APACHE II score to the hospital mortality was 0.62 (95% CI, 0.44-0.79). In conclusion, not only the APACHE II score in neurosurgical patients indicated low severity, but its performance to predict hospital mortality was also inferior. Additional studies of predicting mortality among these critical patients should be undertaken.
Keywords: APACHE; Hospital mortality; Intensive care units; Length of stay; Severity of illness index.
Figures
Similar articles
-
Evaluation of predictive ability of APACHE II system and hospital outcome in Canadian intensive care unit patients.Crit Care Med. 1995 Jul;23(7):1177-83. doi: 10.1097/00003246-199507000-00005. Crit Care Med. 1995. PMID: 7600824
-
Verification of the Acute Physiology and Chronic Health Evaluation scoring system in a Hong Kong intensive care unit.Crit Care Med. 1993 May;21(5):698-705. doi: 10.1097/00003246-199305000-00013. Crit Care Med. 1993. PMID: 8482091
-
A comparison of the Acute Physiology and Chronic Health Evaluation (APACHE) II score and the Trauma-Injury Severity Score (TRISS) for outcome assessment in intensive care unit trauma patients.Crit Care Med. 1996 Oct;24(10):1642-8. doi: 10.1097/00003246-199610000-00007. Crit Care Med. 1996. PMID: 8874299
-
Severity scores in respiratory intensive care: APACHE II predicted mortality better than SAPS II.Respir Care. 1995 Oct;40(10):1042-7. Respir Care. 1995. PMID: 10152703 Review.
-
Predicting outcome in critical care: the current status of the APACHE prognostic scoring system.Can J Anaesth. 1991 Apr;38(3):374-83. doi: 10.1007/BF03007629. Can J Anaesth. 1991. PMID: 2036699 Review.
Cited by
-
Efficacy and safety of MAS825 (anti-IL-1β/IL-18) in COVID-19 patients with pneumonia and impaired respiratory function.Clin Exp Immunol. 2023 Oct 13;213(3):265-275. doi: 10.1093/cei/uxad065. Clin Exp Immunol. 2023. PMID: 37338154 Free PMC article. Clinical Trial.
-
Predictive accuracy of lactate albumin ratio for mortality in intensive care units: a nationwide cohort study.BMJ Open. 2024 Dec 20;14(12):e088926. doi: 10.1136/bmjopen-2024-088926. BMJ Open. 2024. PMID: 39806598 Free PMC article.
-
Acute Kidney Injury in Patients Undergoing Extracorporeal Membrane Oxygenation: A Retrospective Cohort Study.Indian J Crit Care Med. 2024 Jan;28(1):26-29. doi: 10.5005/jp-journals-10071-24612. Indian J Crit Care Med. 2024. PMID: 38510762 Free PMC article.
-
Predictors of Treatment Failure and Mortality among Patients with Septic Shock Treated with Meropenem in the Intensive Care Unit.Malays J Med Sci. 2024 Feb;31(1):76-90. doi: 10.21315/mjms2024.31.1.7. Epub 2024 Feb 28. Malays J Med Sci. 2024. PMID: 38456106 Free PMC article.
-
Clinical Evaluation of Continuous Renal Replacement Therapy Combined with Peritoneal Lavage for Severe Acute Pancreatitis: A Retrospective Cohort Study.Med Sci Monit. 2023 Apr 12;29:e939314. doi: 10.12659/MSM.939314. Med Sci Monit. 2023. PMID: 37041732 Free PMC article.
References
-
- Park SK, Chun HJ, Kim DW, Im TH, Hong HJ, Yi HJ. Acute Physiology and Chronic Health Evaluation II and Simplified Acute Physiology Score II in predicting hospital mortality of neurosurgical intensive care unit patients. J Korean Med Sci. 2009;24:420–6. 10.3346/jkms.2009.24.3.420 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical