

Congenital Adrenal Hyperplasia Presenting as Pulseless Ventricular Tachycardia in a Neonate
- PMID: 31363431
- PMCID: PMC6663285
- DOI: 10.7759/cureus.4749
Congenital Adrenal Hyperplasia Presenting as Pulseless Ventricular Tachycardia in a Neonate
Abstract
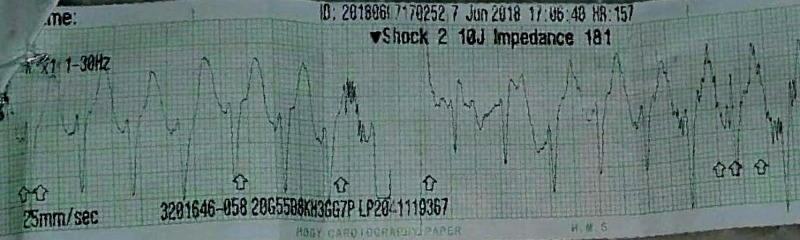
Congenital adrenal hyperplasia (CAH) comprises a group of autosomal recessive inherited disorders that arise due to defects in one of the enzymes of steroidogenesis pathway in the adrenal glands. Ninety-five percent of the cases occur due to deficiency in 21-hydroxylase (21-OH). Clinically, CAH due to 21-OH deficiency presents in two distinct forms, classic CAH and non-classic CAH. Females with classical forms present with genial ambiguity while the presentation in males is more subtle with severe electrolyte disturbances being the initial manifestation in many cases. Arrhythmias are a rare manifestation of CAH. We report the case of an 18-day-old male child who presented with pulseless ventricular tachycardia and was later diagnosed with congenital adrenal hyperplasia based on the laboratory findings of elevated 17-hydroxyprogesterone (17-OHP) levels. Our case reveals that fatal arrhythmias such as a pulseless ventricular tachycardia can be the primary manifestation of the adrenal insufficiency of CAH even in the absence of any physical findings and hence clinicians should always maintain a strong suspicion for CAH in any child presenting with unexplained arrhythmia. Furthermore, this case also highlights the need for CAH screening in neonates so that the appropriate hormone replacement can be initiated before the development of life-threatening adrenal crisis.
Keywords: congenital adrenal hyperplasia; pulseless ventricular tachycardia.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Devastating salt-wasting crisis in a four-month-old male child with congenital adrenal hyperplasia, highlighting the essence of neonatal screening.Clin Case Rep. 2022 Jul 11;10(7):e6010. doi: 10.1002/ccr3.6010. eCollection 2022 Jul. Clin Case Rep. 2022. PMID: 35846927 Free PMC article.
-
[Congenital adrenal hyperplasia].Med Pregl. 1999 Nov-Dec;52(11-12):447-54. Med Pregl. 1999. PMID: 10748766 Review. Croatian.
-
An update of congenital adrenal hyperplasia.Ann N Y Acad Sci. 2004 Dec;1038:14-43. doi: 10.1196/annals.1315.009. Ann N Y Acad Sci. 2004. PMID: 15838095
-
[Diffuse hypertrichosis revealing non-classical congenital adrenal hyperplasia].Ann Dermatol Venereol. 2018 Apr;145(4):270-277. doi: 10.1016/j.annder.2018.02.003. Epub 2018 Mar 7. Ann Dermatol Venereol. 2018. PMID: 29525066 French.
-
Congenital adrenal hyperplasia: clinical symptoms and diagnostic methods.Acta Biochim Pol. 2018;65(1):25-33. doi: 10.18388/abp.2017_2343. Epub 2018 Mar 15. Acta Biochim Pol. 2018. PMID: 29543924 Review.
References
-
- Future directions in the study and management of congenital adrenal hyperplasia due to 21-hydroxylase deficiency. Merke DP, Bornstein SR, Avila NA, Chrousos GP. Ann Intern Med. 2002;136:320–334. - PubMed
-
- Recent advances in diagnosis, treatment, and outcome of congenital adrenal hyperplasia due to 21-hydroxylase deficiency. Riepe FG, Sippell WG. Rev Endocr Metab Disord. 2007;8:349–363. - PubMed
-
- Congenital adrenal hyperplasia. Speiser PW, White PC. N Engl J Med. 2003;349:776–788. - PubMed
-
- Congenital adrenal hyperplasia. Merke DP, Bornstein SR. Lancet. 2005;365:2125–2136. - PubMed
Publication types
LinkOut - more resources
Full Text Sources