

Point of care renal ultrasonography for the busy nephrologist: A pictorial review
- PMID: 31363461
- PMCID: PMC6656660
- DOI: 10.5527/wjn.v8.i3.44
Point of care renal ultrasonography for the busy nephrologist: A pictorial review
Abstract
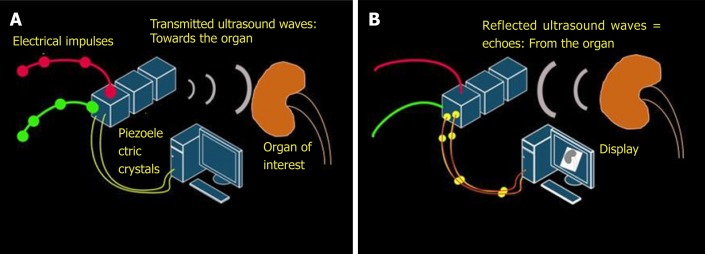
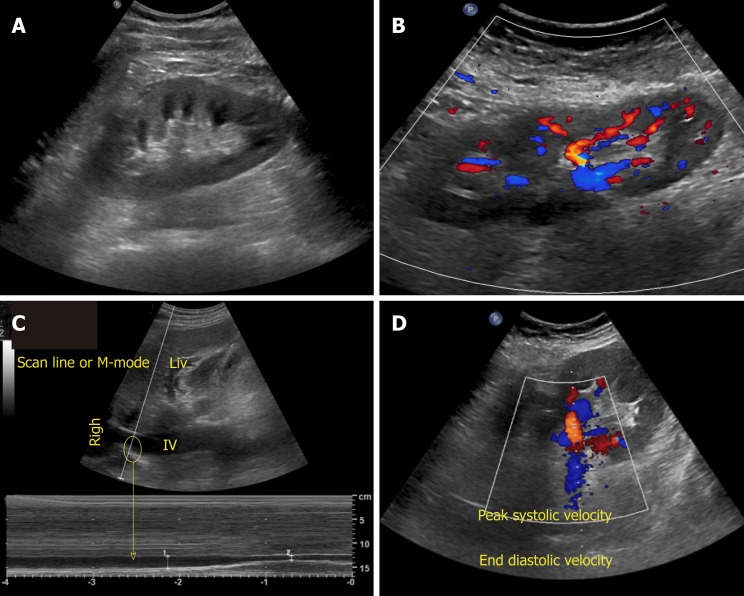
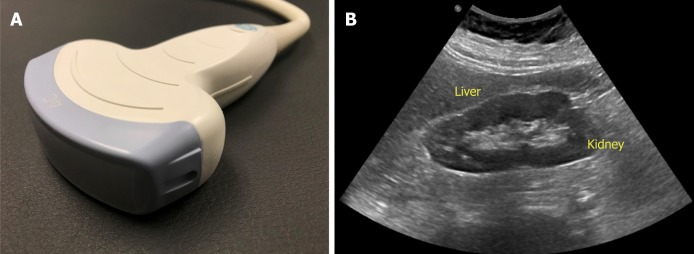
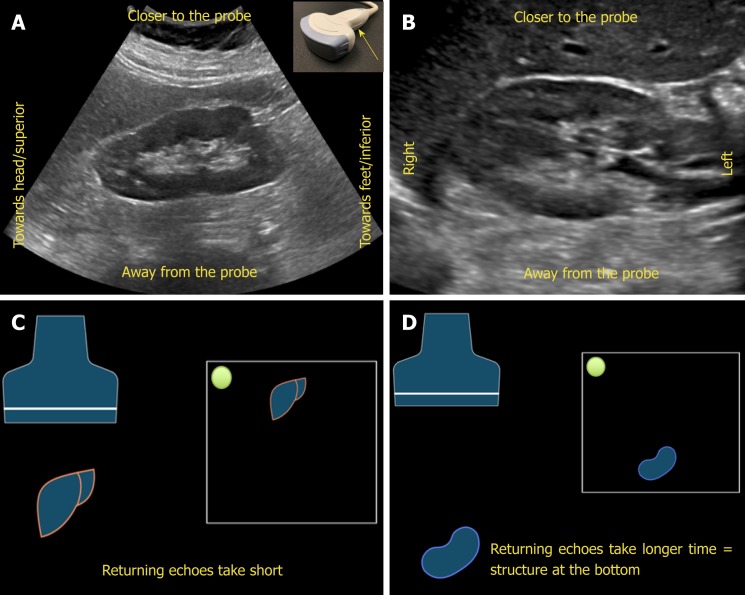
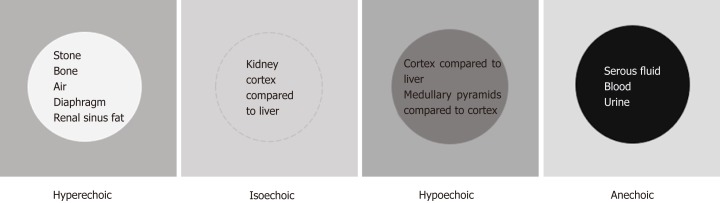
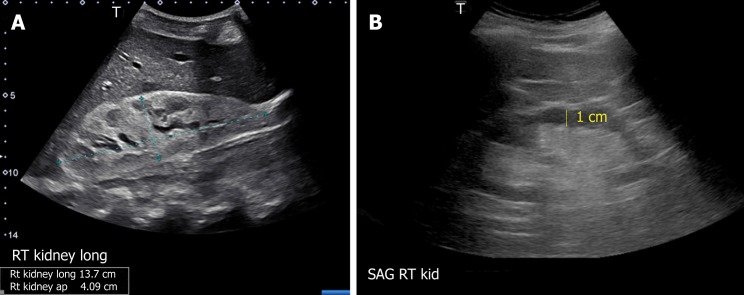
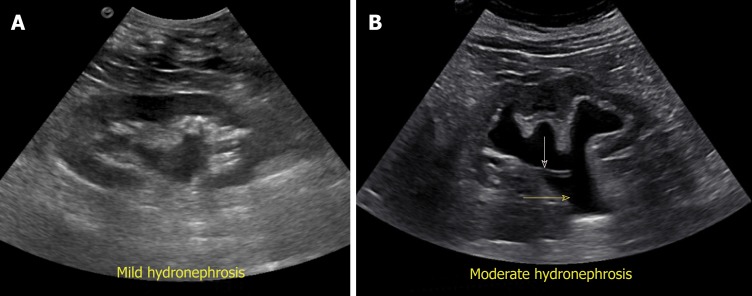
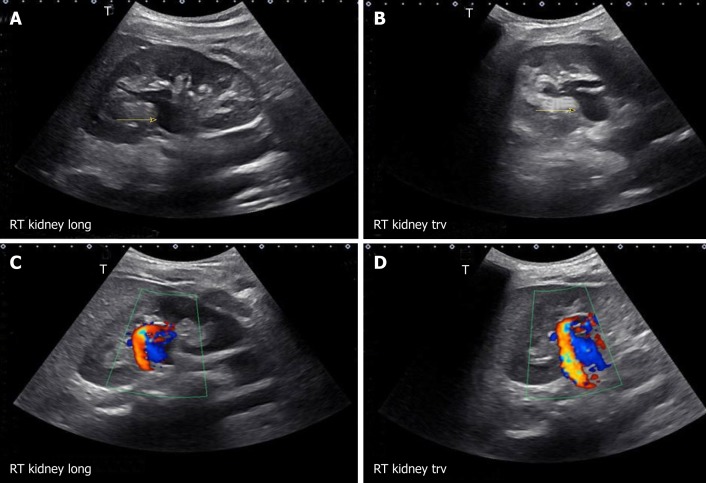
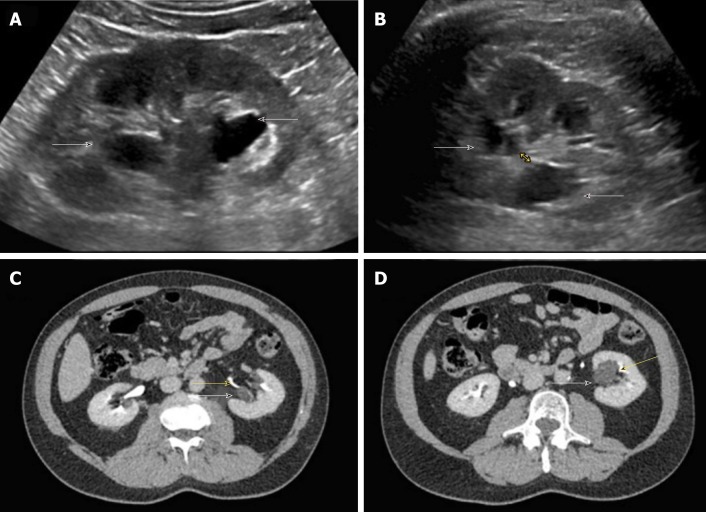
The application of bedside ultrasonography in routine clinical practice has dramatically evolved over the last few decades and will likely continue to grow as technological advances lead to enhanced portability and affordability of the equipment. Despite mounting interest, most nephrology fellowship training programs do not offer formal training in renal ultrasonography and there is inertia among practicing nephrologists to adopt this skill as a practice-changing advancement. Lack of familiarity with the topic is considered a key reason for this inertia. Understanding of basic ultrasound physics, instrumentation, principles of optimal image acquisition and interpretation is critical for enhanced efficiency and patient safety while using this tool. Herein, we provide a brief overview of the basic principles of diagnostic renal ultrasonography as well as introduction to common sonographic pathologies encountered in day-to-day nephrology practice with illustrative images.
Keywords: Cyst; Hydronephrosis; Kidney; Point of care; Stone; Ultrasound.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflicts of interest to declare.
Figures
References
-
- Narula J, Chandrashekhar Y, Braunwald E. Time to Add a Fifth Pillar to Bedside Physical Examination: Inspection, Palpation, Percussion, Auscultation, and Insonation. JAMA Cardiol. 2018;3:346–350. - PubMed
-
- Koratala A, Bhattacharya D, Kazory A. Helping patients and the profession: Nephrology-oriented point-of-care ultrasound program for internal medicine residents. Clin Nephrol. 2018 - PubMed
-
- Lieu D. Ultrasound physics and instrumentation for pathologists. Arch Pathol Lab Med. 2010;134:1541–1556. - PubMed
-
- Enriquez JL, Wu TS. An introduction to ultrasound equipment and knobology. Crit Care Clin. 2014;30:25–45, v. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
