

Clinical differentiation of acute appendicitis and right colonic diverticulitis: A case-control study
- PMID: 31363467
- PMCID: PMC6656680
- DOI: 10.12998/wjcc.v7.i12.1393
Clinical differentiation of acute appendicitis and right colonic diverticulitis: A case-control study
Abstract
Background: Acute right colonic diverticulitis (ARCD) is an important differential diagnosis of acute appendicitis (AA) in Asian countries because of the unusually high prevalence of right colonic diverticula. Due to qualitative improvement and the high penetration rate of computed tomography (CT) scanning in Japan, differentiation of ARCD and AA mainly depends on this modality. But cost, limited availability, and concern for radiation exposure make CT scanning problematic. Differential findings of ARCD from AA are based on several small studies that used univariate comparisons from Korea and Taiwan. Previous studies on clinical and laboratory differences between AA and ARCD are limited.
Aim: To determine clinical differences between AA and ARCD for differentiation of these two diagnoses by creating a logistic regression model.
Methods: We performed an exploratory single-center retrospective case-control study evaluating 369 Japanese patients (age ≥ 16 years), 236 (64.0%) with AA and 133 (36.0%) with ARCD, who were hospitalized between 2012 and 2016. Diagnoses were confirmed by CT images. We compared age, sex, onset-to-visit interval, epigastric/periumbilical pain, right lower quadrant (RLQ) pain, nausea/vomiting, diarrhea, anorexia, medical history, body temperature, blood pressure, heart rate, RLQ tenderness, peritoneal signs, leukocyte count, and levels of serum creatinine, serum C-reactive protein (CRP), and serum alanine aminotrans-ferase. We subsequently performed logistic regression analysis for differentiating AA from ARCD based on the results of the univariate analyses.
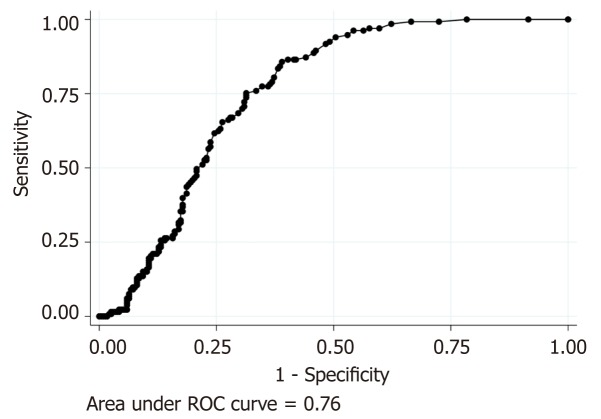
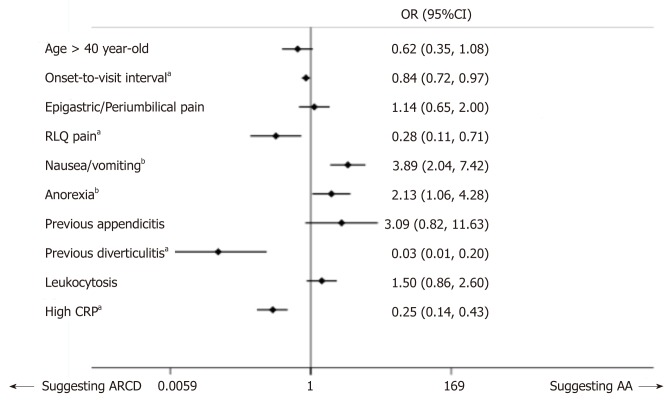
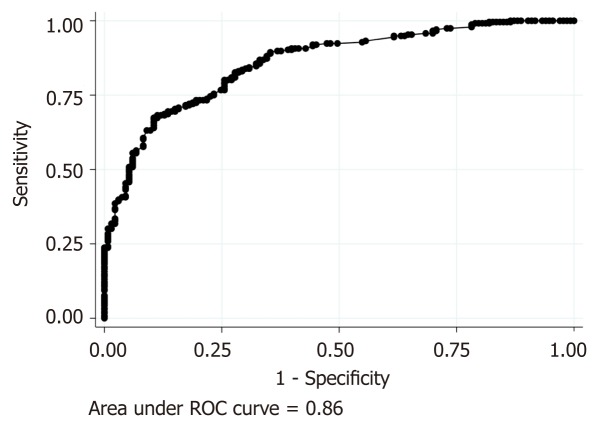
Results: In the AA and ARCD groups, median ages were 35.5 and 41.0 years, respectively (p=0.011); median onset-to-visit intervals were 1 [interquartile range (IQR): 0-1] and 2 (IQR: 1-3) days, respectively (P < 0.001); median leukocyte counts were 12600 and 11500/mm3, respectively (P = 0.002); and median CRP levels were 1.1 (IQR: 0.2-4.1) and 4.9 (IQR: 2.9-8.5) mg/dL, respectively (P < 0.001). In the logistic regression model, odds ratios (ORs) were significantly high in nausea/vomiting (OR: 3.89, 95%CI: 2.04-7.42) and anorexia (OR: 2.13, 95%CI: 1.06-4.28). ORs were significantly lower with a longer onset-to-visit interval (OR: 0.84, 95%CI: 0.72-0.97), RLQ pain (OR: 0.28, 95%CI: 0.11-0.71), history of diverticulitis (OR: 0.034, 95%CI: 0.005-0.20), and CRP level > 3.0 mg/dL (OR: 0.25, 95%CI: 0.14-0.43). The regression model showed good calibration, discrimination, and optimism.
Conclusion: Clinical findings can differentiate AA and ARCD before imaging studies; nausea/vomiting and anorexia suggest AA, and longer onset-to-visit interval, RLQ pain, previous diverticulitis, and CRP level > 3.0 mg/dL suggest ARCD.
Keywords: Abdominal pain; Acute abdomen; Appendicitis; C-reactive protein; Clinical difference; Diverticulitis; Right lower quadrant pain.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Clinical Difference between Acute Appendicitis and Acute Right-Sided Colonic Diverticulitis.Emerg Med Int. 2020 Sep 1;2020:4947192. doi: 10.1155/2020/4947192. eCollection 2020. Emerg Med Int. 2020. PMID: 32953179 Free PMC article.
-
Clinical prediction of complicated appendicitis: A case-control study utilizing logistic regression.World J Clin Cases. 2020 Jun 6;8(11):2127-2136. doi: 10.12998/wjcc.v8.i11.2127. World J Clin Cases. 2020. PMID: 32548142 Free PMC article.
-
Children presenting at the emergency department with right lower quadrant pain.Kaohsiung J Med Sci. 2009 Jan;25(1):1-9. doi: 10.1016/S1607-551X(09)70033-6. Kaohsiung J Med Sci. 2009. PMID: 19289311 Free PMC article.
-
Cecal diverticulitis: a case report and review of the current literature.Int Surg. 2001 Jul-Sep;86(3):191-4. Int Surg. 2001. PMID: 11996078 Review.
-
Ultrasound of colon diverticulitis.Dig Dis. 2012;30(1):56-9. doi: 10.1159/000336620. Epub 2012 May 3. Dig Dis. 2012. PMID: 22572686 Review.
Cited by
-
Acute appendicitis-advances and controversies.World J Gastrointest Surg. 2021 Nov 27;13(11):1293-1314. doi: 10.4240/wjgs.v13.i11.1293. World J Gastrointest Surg. 2021. PMID: 34950421 Free PMC article. Review.
-
Clinical Difference between Acute Appendicitis and Acute Right-Sided Colonic Diverticulitis.Emerg Med Int. 2020 Sep 1;2020:4947192. doi: 10.1155/2020/4947192. eCollection 2020. Emerg Med Int. 2020. PMID: 32953179 Free PMC article.
-
Right-sided acute diverticulitis in the West: experience at a university hospital in Argentina.Ann Coloproctol. 2023 Apr;39(2):123-130. doi: 10.3393/ac.2021.00402.0057. Epub 2021 Nov 24. Ann Coloproctol. 2023. PMID: 34814235 Free PMC article.
References
-
- Narasaka T, Watanabe H, Yamagata S, Munakata A, Tajima T. Statistical analysis of diverticulosis of the colon. Tohoku J Exp Med. 1975;115:271–275. - PubMed
-
- Chan CC, Lo KK, Chung EC, Lo SS, Hon TY. Colonic diverticulosis in Hong Kong: distribution pattern and clinical significance. Clin Radiol. 1998;53:842–844. - PubMed
-
- Matsushima K. Management of right-sided diverticulitis: A retrospective review from a hospital in Japan. Surg Today. 2010;40:321–325. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
