

Respiratory syncytial virus hospitalisations among young children: a data linkage study
- PMID: 31364578
- PMCID: PMC6805750
- DOI: 10.1017/S0950268819001377
Respiratory syncytial virus hospitalisations among young children: a data linkage study
Erratum in
-
Respiratory syncytial virus hospitalisations among young children: a data linkage study - Erratum.Epidemiol Infect. 2020 Aug 28;148:e179. doi: 10.1017/S0950268820001612. Epidemiol Infect. 2020. PMID: 32856578 Free PMC article. No abstract available.
Abstract
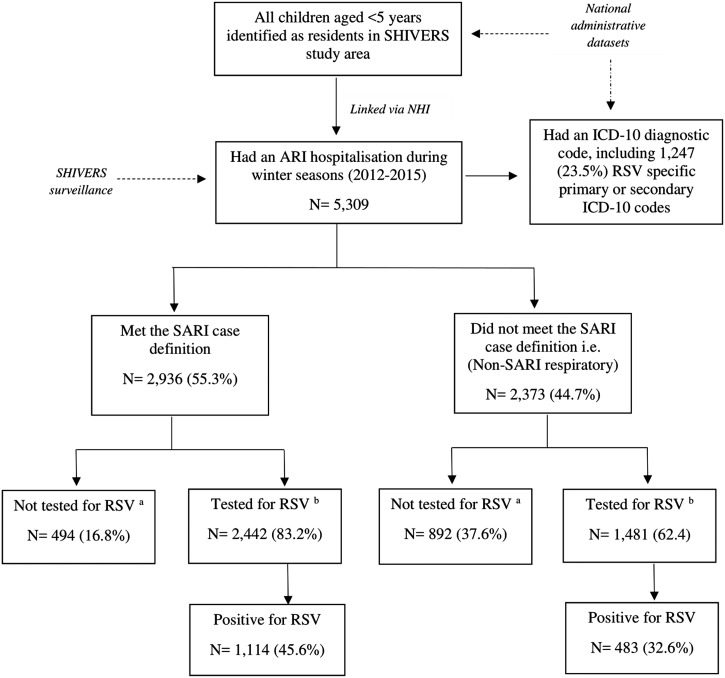
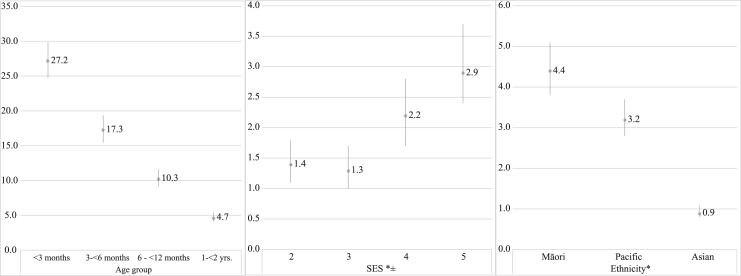
We aimed to provide comprehensive estimates of laboratory-confirmed respiratory syncytial virus (RSV)-associated hospitalisations. Between 2012 and 2015, active surveillance of acute respiratory infection (ARI) hospitalisations during winter seasons was used to estimate the seasonal incidence of laboratory-confirmed RSV hospitalisations in children aged <5 years in Auckland, New Zealand (NZ). Incidence rates were estimated by fine age group, ethnicity and socio-economic status (SES) strata. Additionally, RSV disease estimates determined through active surveillance were compared to rates estimated from hospital discharge codes. There were 5309 ARI hospitalisations among children during the study period, of which 3923 (73.9%) were tested for RSV and 1597 (40.7%) were RSV-positive. The seasonal incidence of RSV-associated ARI hospitalisations, once corrected for non-testing, was 6.1 (95% confidence intervals 5.8-6.4) per 1000 children <5 years old. The highest incidence was among children aged <3 months. Being of indigenous Māori or Pacific ethnicity or living in a neighbourhood with low SES independently increased the risk of an RSV-associated hospitalisation. RSV hospital discharge codes had a sensitivity of 71% for identifying laboratory-confirmed RSV cases. RSV infection is a leading cause of hospitalisation among children in NZ, with significant disparities by ethnicity and SES. Our findings highlight the need for effective RSV vaccines and therapies.
Keywords: Infectious disease epidemiology; paediatrics; respiratory infections; respiratory syncytial virus.
Conflict of interest statement
NP, ECN, QSH are currently contracted by GlaxoSmithKline on an RSV surveillance project.
Figures

Similar articles
-
Comparison of the Burden and Temporal Pattern of Hospitalisations Associated With Respiratory Syncytial Virus (RSV) Before and After COVID-19 in New Zealand.Influenza Other Respir Viruses. 2024 Jul;18(7):e13346. doi: 10.1111/irv.13346. Influenza Other Respir Viruses. 2024. PMID: 38980967 Free PMC article.
-
Incidence and seasonality of respiratory syncytial virus hospitalisations in young children in Denmark, 2010 to 2015.Euro Surveill. 2018 Jan;23(3):17-00163. doi: 10.2807/1560-7917.ES.2018.23.3.17-00163. Euro Surveill. 2018. PMID: 29386093 Free PMC article.
-
Hospital-based surveillance of respiratory syncytial virus in Central Queensland.Commun Dis Intell (2018). 2025 May 19;49. doi: 10.33321/cdi.2025.49.041. Commun Dis Intell (2018). 2025. PMID: 40383523
-
Burden of respiratory syncytial virus (RSV) infection in Germany: a systematic review.BMC Infect Dis. 2024 Aug 20;24(1):844. doi: 10.1186/s12879-024-09758-3. BMC Infect Dis. 2024. PMID: 39164625 Free PMC article.
-
Respiratory Syncytial Virus associated hospitalisations in children up to 6 years of age in Italy: a systematic review.Ann Ig. 2025 Mar-Apr;37(2):241-254. doi: 10.7416/ai.2024.2664. Epub 2024 Nov 7. Ann Ig. 2025. PMID: 39526552
Cited by
-
Temporal Variations in Respiratory Syncytial Virus Epidemics, by Virus Subtype, 4 Countries.Emerg Infect Dis. 2021 May;27(5):1537-1540. doi: 10.3201/eid2705.204615. Emerg Infect Dis. 2021. PMID: 33900190 Free PMC article.
-
Estimating the Incidence of First RSV Hospitalization in Children Born in Ontario, Canada.J Pediatric Infect Dis Soc. 2023 Jul 31;12(7):421-430. doi: 10.1093/jpids/piad045. J Pediatric Infect Dis Soc. 2023. PMID: 37335754 Free PMC article.
-
Epidemiology of Respiratory Syncytial Virus-Related Hospitalization Over a 5-Year Period in Italy: Evaluation of Seasonality and Age Distribution Before Vaccine Introduction.Vaccines (Basel). 2020 Jan 4;8(1):15. doi: 10.3390/vaccines8010015. Vaccines (Basel). 2020. PMID: 31947976 Free PMC article.
-
Hospitalization rate of respiratory syncytial virus-associated acute lower respiratory infection among young children in Suzhou, China, 2010-2014.Influenza Other Respir Viruses. 2022 Jul;16(4):789-799. doi: 10.1111/irv.12958. Epub 2022 Jan 5. Influenza Other Respir Viruses. 2022. PMID: 34989118 Free PMC article.
-
Clinical and economic burden of respiratory syncytial virus in Spanish children: the BARI study.BMC Infect Dis. 2022 Sep 29;22(1):759. doi: 10.1186/s12879-022-07745-0. BMC Infect Dis. 2022. PMID: 36175846 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
