

Association With Hospitalization and All-Cause Discontinuation Among Patients With Schizophrenia on Clozapine vs Other Oral Second-Generation Antipsychotics: A Systematic Review and Meta-analysis of Cohort Studies
- PMID: 31365048
- PMCID: PMC6669790
- DOI: 10.1001/jamapsychiatry.2019.1702
Association With Hospitalization and All-Cause Discontinuation Among Patients With Schizophrenia on Clozapine vs Other Oral Second-Generation Antipsychotics: A Systematic Review and Meta-analysis of Cohort Studies
Abstract
Importance: Recent meta-analyses of randomized clinical trials (RCTs) comparing clozapine with nonclozapine second-generation antipsychotics (NC-SGAs) in schizophrenia have challenged clozapine's superiority in treatment-resistant patients. However, patients in RCTs are not necessarily generalizable to those in clinical practice.
Objective: To conduct a systematic review and meta-analysis to compare various outcomes of clozapine vs oral NC-SGAs in cohort studies.
Data sources: Systematic literature search in PubMed, PsycINFO, and CINAHL without language restriction from database inception until December 17, 2018.
Study selection: Nonrandomized cohort studies reporting effectiveness and/or safety outcomes comparing clozapine with NC-SGAs in schizophrenia or schizoaffective disorder.
Data extraction and synthesis: Independent investigators assessed studies and extracted data. Using a random-effects model, the study calculated risk ratio (RR) unadjusted for covariates and follow-up duration, number needed to treat/number needed to harm (NNT/NNH) for dichotomous data, and standardized mean difference (SMD) or mean difference (MD) for continuous data.
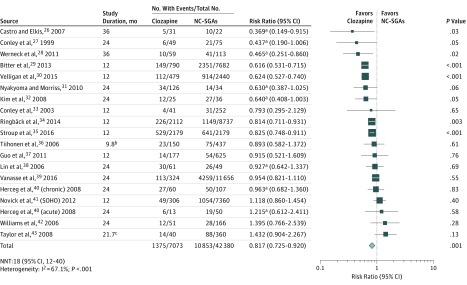
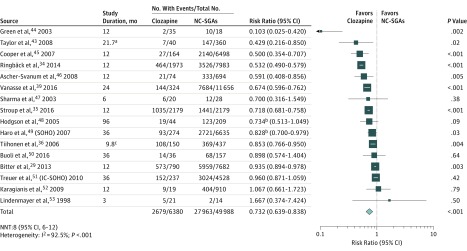
Main outcomes and measures: Coprimary outcomes were hospitalization and all-cause discontinuation. Secondary outcomes included all effectiveness and safety outcomes reported in at least 3 analyzable studies.
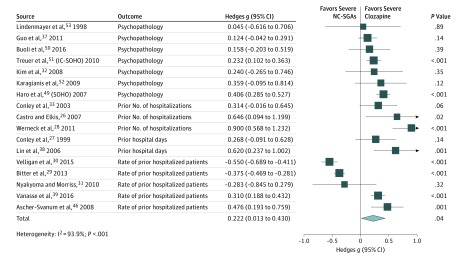
Results: Of 8446 hits, 68 articles from 63 individual cohort studies (n = 109 341) (60.3% male; mean [SD] age of 38.8 [6.5] years, illness duration of 11.0 [5.1] years, and study duration of 19.1 [23.3] months) were meta-analyzed. Compared with NC-SGAs, despite greater illness severity (17 studies [n = 38 766]; Hedges g, 0.222; 95% CI, 0.013-0.430; P = .04), clozapine was significantly associated with lower hospitalization risk (19 studies [n = 49 453]; RR, 0.817; 95% CI, 0.725-0.920; P = .001; NNT, 18; 95% CI, 12-40) and all-cause discontinuation (16 studies [n = 56 368]; RR, 0.732; 95% CI, 0.639-0.838; P < .001; NNT, 8; 95% CI, 6-12). Associations were statistically significant for comparisons with quetiapine fumarate and aripiprazole regarding hospitalization and all NC-SGAs, except aripiprazole, for all-cause discontinuation. Clozapine was also significantly associated with better outcomes regarding overall symptoms (SMD, -0.302; 95% CI, -0.572 to -0.032; P = .03) and Clinical Global Impressions scale severity (SMD, -1.182; 95% CI, -2.243 to -0.122; P = .03). Clozapine was significantly associated with increases in body weight (MD, 1.70; 95% CI, 0.31-3.08 kg; P = .02), body mass index (MD, 0.96; 95% CI, 0.24-1.68; P = .009), and type 2 diabetes (RR, 1.777; 95% CI, 1.229-2.570; P = .002; NNH, 27; 95% CI, 13-90).
Conclusions and relevance: In cohort studies, despite more severely ill patients being treated with clozapine, use of clozapine was associated with better key efficacy outcomes and higher cardiometabolic-related risk outcomes vs NC-SGAs.
Conflict of interest statement
Figures
Comment in
-
Clozapine and Evidence-Based Psychopharmacology for Schizophrenia.JAMA Psychiatry. 2019 Oct 1;76(10):1007-1008. doi: 10.1001/jamapsychiatry.2019.1656. JAMA Psychiatry. 2019. PMID: 31365031 No abstract available.
References
-
- National Institute for Health and Care Excellence Psychosis and schizophrenia in adults: prevention and management. Clinical Guideline CG178. https://www.nice.org.uk/guidance/cg178. Published February 2014. Updated March 2014. Accessed August 12, 2017.
-
- Falkai P, Wobrock T, Lieberman J, Glenthoj B, Gattaz WF, Möller HJ; WFSBP Task Force on Treatment Guidelines for Schizophrenia . World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of schizophrenia, part 1: acute treatment of schizophrenia. World J Biol Psychiatry. 2005;6(3):132-191. doi: 10.1080/15622970510030090 - DOI - PubMed
-
- Lehman AF, Lieberman JA, Dixon LB, et al. American Psychiatric Association; Steering Committee on Practice Guidelines. Practice guideline for the treatment of patients with schizophrenia, second edition. Am J Psychiatry 2004;161(2)(suppl):1-56. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
