Assessment of Therapeutic Interventions and Lung Protective Ventilation in Patients With Moderate to Severe Acute Respiratory Distress Syndrome: A Systematic Review and Network Meta-analysis
- PMID: 31365111
- PMCID: PMC6669780
- DOI: 10.1001/jamanetworkopen.2019.8116
Assessment of Therapeutic Interventions and Lung Protective Ventilation in Patients With Moderate to Severe Acute Respiratory Distress Syndrome: A Systematic Review and Network Meta-analysis
Abstract
Importance: A number of interventions are available to manage patients with moderate to severe acute respiratory distress syndrome (ARDS). However, the associations of currently available ventilatory strategies and adjunctive therapies with mortality are uncertain.
Objectives: To compare and rank different therapeutic strategies to identify the best intervention associated with a reduction in mortality in adult patients with moderate to severe ARDS.
Data sources: An electronic search of MEDLINE, MEDLINE In-Process/ePubs Ahead of Print, Embase, Cochrane Controlled Clinical Trial Register (Central), PubMed, and CINAHL was conducted, from database inception to May 29, 2019.
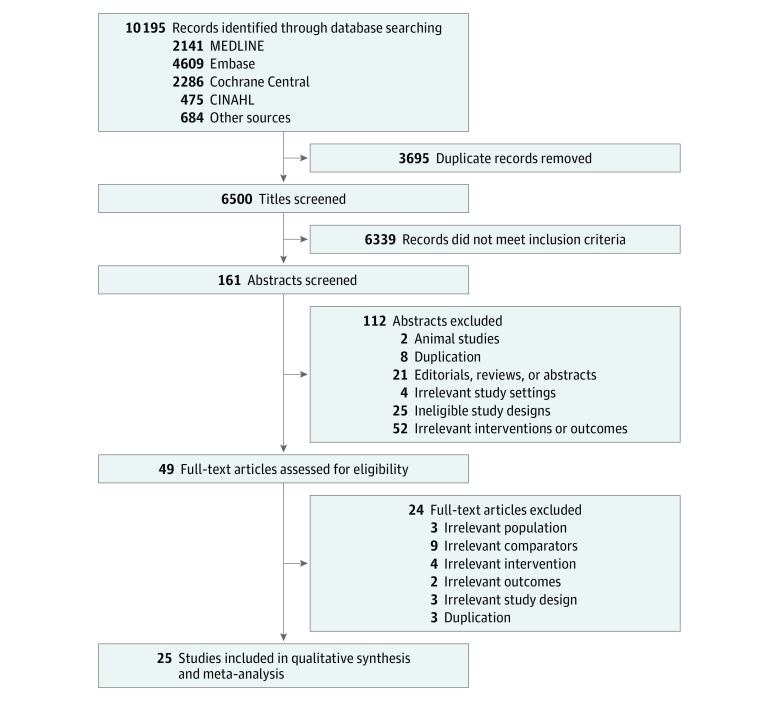
Study selection: Randomized clinical trials of interventions for adults with moderate to severe ARDS that used lung protective ventilation. No language restrictions were applied.
Data extraction and synthesis: Data were independently extracted by 2 reviewers and synthesized with Bayesian random-effects network meta-analyses.
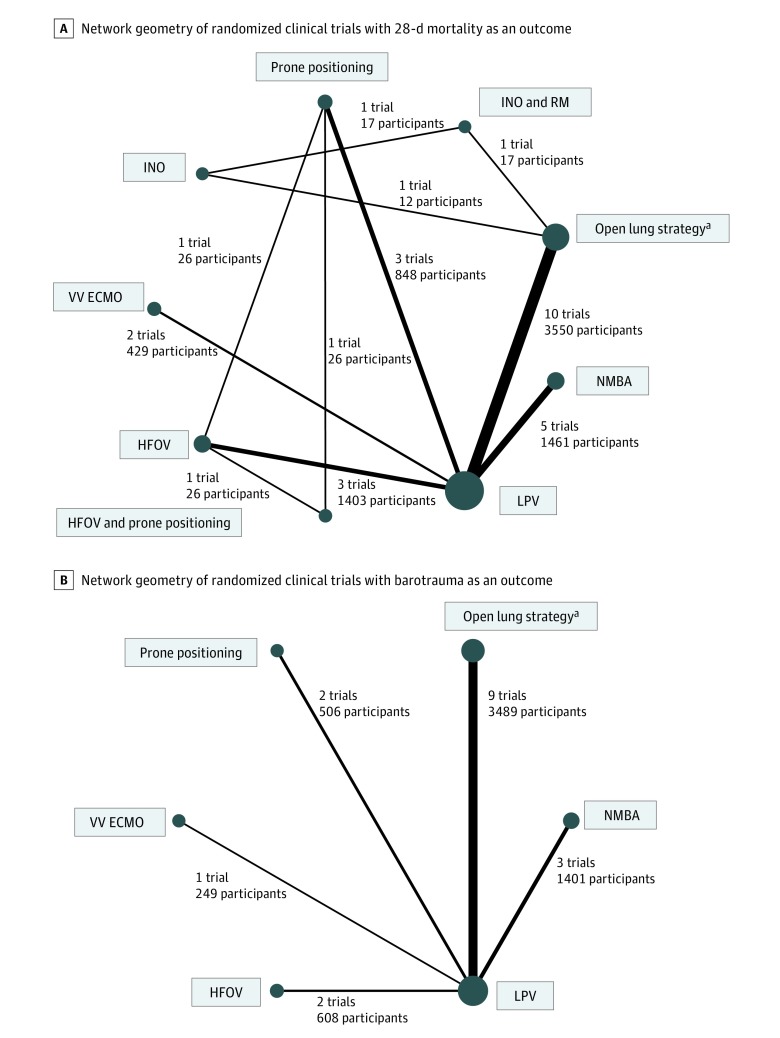
Main outcomes and measures: The primary outcome was 28-day mortality. Barotrauma was a secondary outcome.
Results: Among 25 randomized clinical trials evaluating 9 interventions, 2686 of 7743 patients (34.6%) died within 28 days. Compared with lung protective ventilation alone, prone positioning and venovenous extracorporeal membrane oxygenation were associated with significantly lower 28-day mortality (prone positioning: risk ratio, 0.69; 95% credible interval, 0.48-0.99; low quality of evidence; venovenous extracorporeal membrane oxygenation: risk ratio, 0.60; 95% credible interval, 0.38-0.93; moderate quality of evidence). These 2 interventions had the highest ranking probabilities, although they were not significantly different from each other. Among 18 trials reporting on barotrauma, 448 of 6258 patients (7.2%) experienced this secondary outcome. No intervention was superior to any other in reducing barotrauma, and each represented low to very low quality of evidence.
Conclusions and relevance: This network meta-analysis supports the use of prone positioning and venovenous extracorporeal membrane oxygenation in addition to lung protective ventilation in patients with ARDS. Moreover, venovenous extracorporeal membrane oxygenation may be considered as an early strategy for adults with severe ARDS receiving lung protective ventilation.
Conflict of interest statement
Figures