

Effect of staged crestal maxillary sinus augmentation: A case series
- PMID: 31365130
- PMCID: PMC7065142
- DOI: 10.1002/JPER.18-0632
Effect of staged crestal maxillary sinus augmentation: A case series
Abstract
Background: In sinus augmentation, when remaining bone height is ≤5 mm, a lateral window approach is often the preferred choice; nonetheless, patients prefer to have a less invasive approach such as crestal sinus augmentation (CSA). Prior case reports have described the use of various staged approaches of a CSA technique in cases of limited bone height. The aim of this report was to describe the results of a case series in which a two-stage CSA technique was used in patients with 4 to 6 mm of bone height.
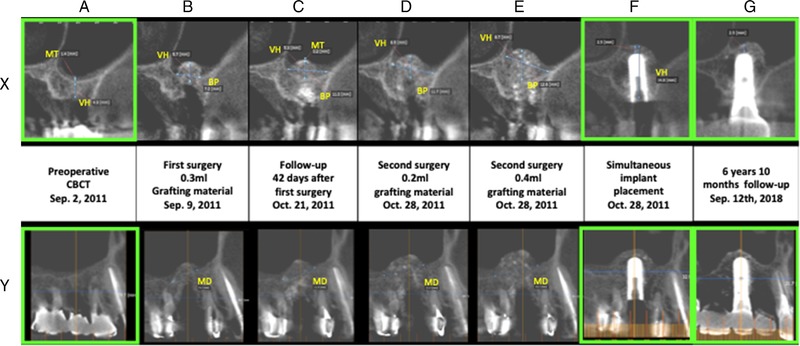
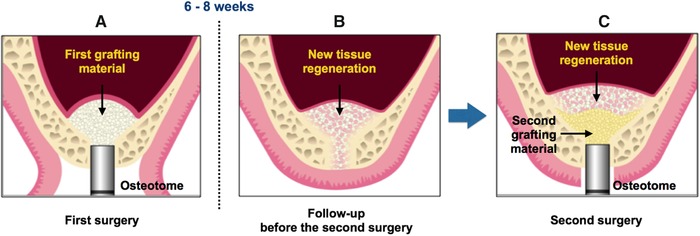
Methods: Nineteen subjects with 28 sinuses of initial vertical bone height of 4 to 6 mm were included in which a two-stage CSA technique was used in place of a lateral window approach. In the first surgery, 0.3 mL graft material was inserted into all sites. In the second surgery, 13 sites were filled with 0.2 mL graft material and remaining 15 sites were filled with 0.4 mL.
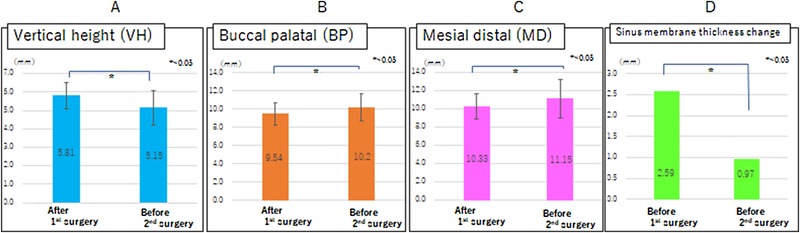
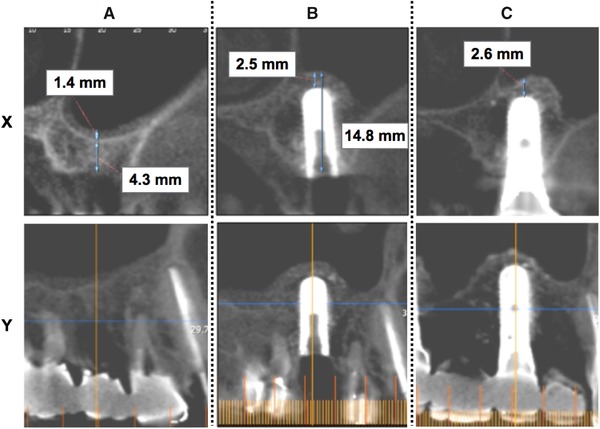
Results: No damage was observed in the maxillary sinus floor membrane after first 0.2 mL filling; however, one case had Schneiderian membrane perforation after filling 0.4 mL. The average elevation height (EH) after first surgery was 5.81 ± 0.7 mm, 5.15 ± 0.91 mm before second surgery, 6.69 ± 0.89 mm with 0.2 mL filling (total 0.5 mL) and 8.11 ± 1.24 mm with 0.4 mL filling (total 0.7 mL). The thickness of maxillary sinus membrane before first surgery was 2.6 ± 2.59 mm; however, it has become 0.97 ± 1.59 mm before second surgery, with a decrease of 1.6 mm estimate.
Conclusion: This case series that assessed outcomes of staged crestal maxillary sinus augmentation was an effective approach to elevating 6 or 8 mm alveolar bone height without causing major membrane perforation. However, the two-stage approach was used in the limited residual bone height (4 to 6 mm) and required two separate surgical procedures.
Keywords: Schneiderian membrane; crestal sinus augmentation; crestal sinus lift; internal sinus lift.
© 2019 The Authors. Journal of Periodontology published by Wiley Periodicals, Inc. on behalf of American Academy of Periodontology.
Figures

Similar articles
-
Osseodensified Crestal Sinus Window Augmentation: An Alternative Procedure to the Lateral Window Technique.J Oral Implantol. 2021 Feb 1;47(1):45-55. doi: 10.1563/aaid-joi-D-19-00288. J Oral Implantol. 2021. PMID: 32663265
-
Crestal Window Sinus Lift and Its Long-Term Clinical Outcomes.Int J Periodontics Restorative Dent. 2020 September/October;40(5):757–764. doi: 10.11607/prd.4292. Epub 2020 Mar 19. Int J Periodontics Restorative Dent. 2020. PMID: 32191779
-
Evaluation of the capability of a new water lift system to reduce the risk of Schneiderian membrane perforation during sinus elevation.Int J Oral Maxillofac Surg. 2011 Aug;40(8):815-20. doi: 10.1016/j.ijom.2011.04.005. Epub 2011 May 18. Int J Oral Maxillofac Surg. 2011. PMID: 21592728 Clinical Trial.
-
Update on Maxillary Sinus Augmentation.Dent Clin North Am. 2021 Jan;65(1):197-210. doi: 10.1016/j.cden.2020.09.013. Epub 2020 Nov 2. Dent Clin North Am. 2021. PMID: 33213709 Review.
-
From maximally to minimally invasive surgery for sinus floor augmentation.Compend Contin Educ Dent. 2013 Jul;34 Spec No:19-24; quiz 25. Compend Contin Educ Dent. 2013. PMID: 24568247 Review.
Cited by
-
Intraoperative complications and early implant failure after transcrestal sinus floor elevation with residual bone height ≤5 mm: A retrospective multicenter study.Clin Oral Implants Res. 2022 Aug;33(8):783-791. doi: 10.1111/clr.13959. Epub 2022 May 29. Clin Oral Implants Res. 2022. PMID: 35578774 Free PMC article.
-
Clinical and radiographic changes following transcrestal sinus augmentation: A scoping review of the last 25 years.Clin Implant Dent Relat Res. 2024 Dec;26(6):1338-1353. doi: 10.1111/cid.13389. Epub 2024 Sep 30. Clin Implant Dent Relat Res. 2024. PMID: 39350529 Free PMC article.
-
Evaluation of crestal sinus floor elevation in cases exhibiting an oblique sinus floor with a residual bone height of 4.0-7.0 mm using Densah burs with simultaneous implant placement: a prospective clinical study.Int J Implant Dent. 2023 Nov 2;9(1):41. doi: 10.1186/s40729-023-00510-1. Int J Implant Dent. 2023. PMID: 37917214 Free PMC article.
-
Modified Osteotome Sinus Floor Elevation Technique for Multiple Edentulous Spaces: A Non-Randomized Controlled Trial.Int J Environ Res Public Health. 2022 Jun 30;19(13):8019. doi: 10.3390/ijerph19138019. Int J Environ Res Public Health. 2022. PMID: 35805687 Free PMC article. Clinical Trial.
References
-
- Boyne PJ, James RA. Grafting of the maxillary sinus floor with autogenous marrow and bone. J Oral Surg. 1980;38:613‐616. - PubMed
-
- Summers RB. A new concept in maxillary implant surgery: the osteotome technique. Compendium. 1994;15:154‐156. - PubMed
-
- Wang HL, Katranji A. ABC sinus augmentation classification. Int J Periodontics Restorative Dent. 2008;28:383‐389. - PubMed
-
- Sonoda T, Harada T, Yamamichi N, Monje A, Wang HL. Association between bone graft volume and maxillary sinus membrane elevation height. Int J Oral Maxillofac Implants. 2017;32:735‐740. - PubMed
-
- Peleg M, Garg AK, Mazor Z. Predictability of simultaneous implant placement in the severely atrophic posterior maxilla: a 9‐year longitudinal experience study of 2132 implants placed into 731 human sinus grafts. Int J Oral Maxillofac Implants. 2006;21:94‐102. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
