

Immediate Transfusion in African Children with Uncomplicated Severe Anemia
- PMID: 31365799
- PMCID: PMC7611152
- DOI: 10.1056/NEJMoa1900105
Immediate Transfusion in African Children with Uncomplicated Severe Anemia
Abstract
Background: The World Health Organization recommends not performing transfusions in African children hospitalized for uncomplicated severe anemia (hemoglobin level of 4 to 6 g per deciliter and no signs of clinical severity). However, high mortality and readmission rates suggest that less restrictive transfusion strategies might improve outcomes.
Methods: In this factorial, open-label, randomized, controlled trial, we assigned Ugandan and Malawian children 2 months to 12 years of age with uncomplicated severe anemia to immediate transfusion with 20 ml or 30 ml of whole-blood equivalent per kilogram of body weight, as determined in a second simultaneous randomization, or no immediate transfusion (control group), in which transfusion with 20 ml of whole-blood equivalent per kilogram was triggered by new signs of clinical severity or a drop in hemoglobin to below 4 g per deciliter. The primary outcome was 28-day mortality. Three other randomizations investigated transfusion volume, postdischarge supplementation with micronutrients, and postdischarge prophylaxis with trimethoprim-sulfamethoxazole.
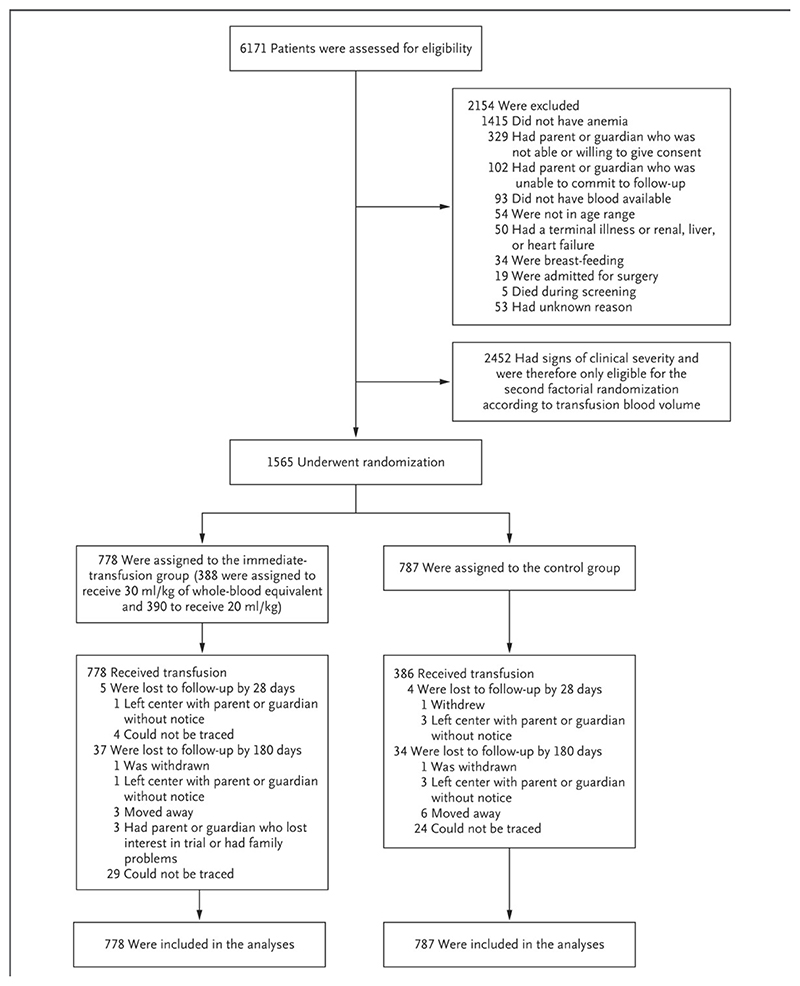
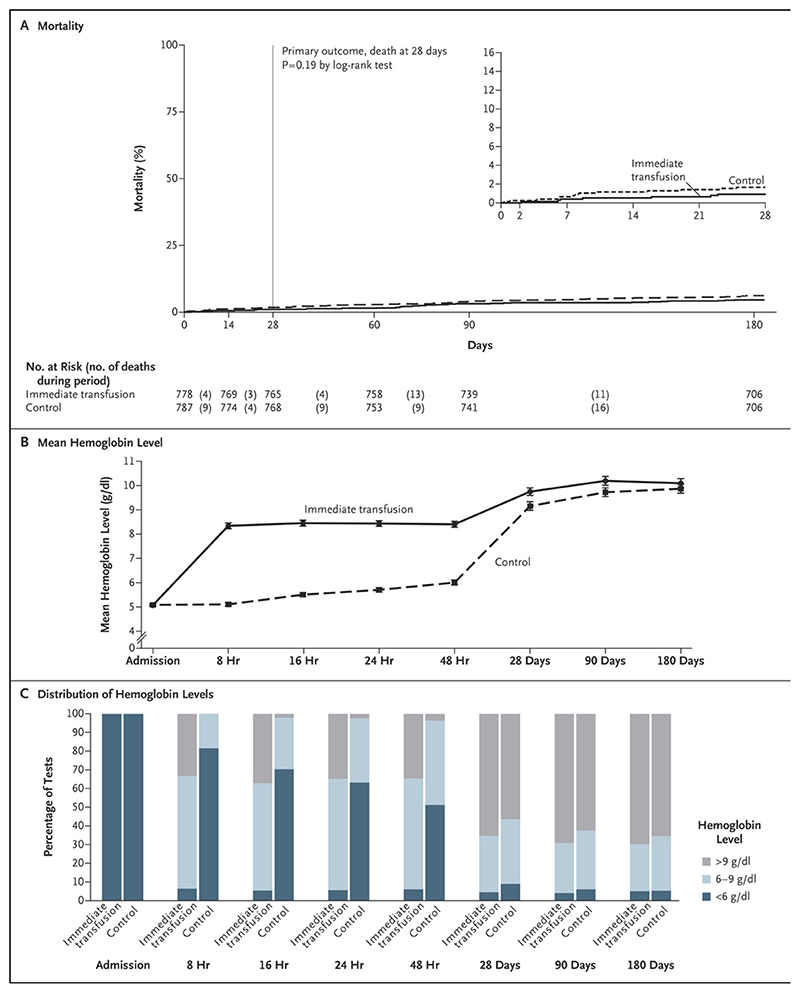
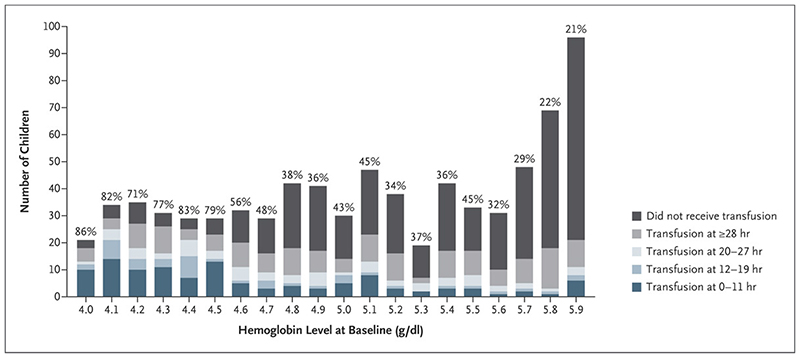
Results: A total of 1565 children (median age, 26 months) underwent randomization, with 778 assigned to the immediate-transfusion group and 787 to the control group; 984 children (62.9%) had malaria. The children were followed for 180 days, and 71 (4.5%) were lost to follow-up. During the primary hospitalization, transfusion was performed in all the children in the immediate-transfusion group and in 386 (49.0%) in the control group (median time to transfusion, 1.3 hours vs. 24.9 hours after randomization). The mean (±SD) total blood volume transfused per child was 314±228 ml in the immediate-transfusion group and 142±224 ml in the control group. Death had occurred by 28 days in 7 children (0.9%) in the immediate-transfusion group and in 13 (1.7%) in the control group (hazard ratio, 0.54; 95% confidence interval [CI], 0.22 to 1.36; P = 0.19) and by 180 days in 35 (4.5%) and 47 (6.0%), respectively (hazard ratio, 0.75; 95% CI, 0.48 to 1.15), without evidence of interaction with other randomizations (P>0.20) or evidence of between-group differences in readmissions, serious adverse events, or hemoglobin recovery at 180 days. The mean length of hospital stay was 0.9 days longer in the control group.
Conclusions: There was no evidence of differences in clinical outcomes over 6 months between the children who received immediate transfusion and those who did not. The triggered-transfusion strategy in the control group resulted in lower blood use; however, the length of hospital stay was longer, and this strategy required clinical and hemoglobin monitoring. (Funded by the Medical Research Council and Department for International Development; TRACT Current Controlled Trials number, ISRCTN84086586.).
Copyright © 2019 Massachusetts Medical Society.
Figures
Comment in
-
Immediate Transfusion and Transfusion Volume in African Children with Severe Anemia.N Engl J Med. 2019 Aug 1;381(5):475-476. doi: 10.1056/NEJMe1908869. N Engl J Med. 2019. PMID: 31365806 No abstract available.
-
Transfusion Timing and Volume in African Children with Severe Anemia.N Engl J Med. 2019 Oct 24;381(17):1686-1687. doi: 10.1056/NEJMc1911668. N Engl J Med. 2019. PMID: 31644853 No abstract available.
-
Liberal vs. Conservative Approach to Timing of Blood Transfusion in Severely Anemic Children: Evidence-based Medicine Viewpoint.Indian Pediatr. 2019 Nov 15;56(11):959-963. Indian Pediatr. 2019. PMID: 31729326 No abstract available.
-
Liberal vs. Conservative Approach to Timing of Blood Transfusion in Severely Anemic Children: Pediatrician's Viewpoint.Indian Pediatr. 2019 Nov 15;56(11):963-964. Indian Pediatr. 2019. PMID: 31729327 No abstract available.
References
-
- Stevens GA, Finucane MM, De-Regil LM, et al. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995-2011: a systematic analysis of population-representative data. Lancet Glob Health. 2013;1:e16-25. - PMC - PubMed
-
- Calis JC, Phiri KS, Faragher EB, et al. Severe anemia in Malawian children. The New England journal of medicine. 2008;358:888–99. - PubMed
-
- Global status report on blood safety and availability 2016. World Health Organization; Geneva: 2017. World Health Organization.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- MC_UU_12023/17/MRC_/Medical Research Council/United Kingdom
- MC_PC_MR/R019258/1/MRC_/Medical Research Council/United Kingdom
- MR/J012483/University Hospital Southampton NHS Foundation Trust/International
- 202800/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- MC_UU_12023/26/MRC_/Medical Research Council/United Kingdom