

The Incidence of Acute Kidney Injury and Associated Hospital Mortality
- PMID: 31366430
- PMCID: PMC6676729
- DOI: 10.3238/arztebl.2019.0397
The Incidence of Acute Kidney Injury and Associated Hospital Mortality
Abstract
Background: Studies from multiple countries have shown that acute kidney injury (AKI) in hospitalized patients is associated with mortality and morbidity. There are no reliable data at present on the incidence and mortality of AKI episodes among hospitalized patients in Germany. The utility of administrative codings of AKI for the identification of AKI episodes is also unclear.
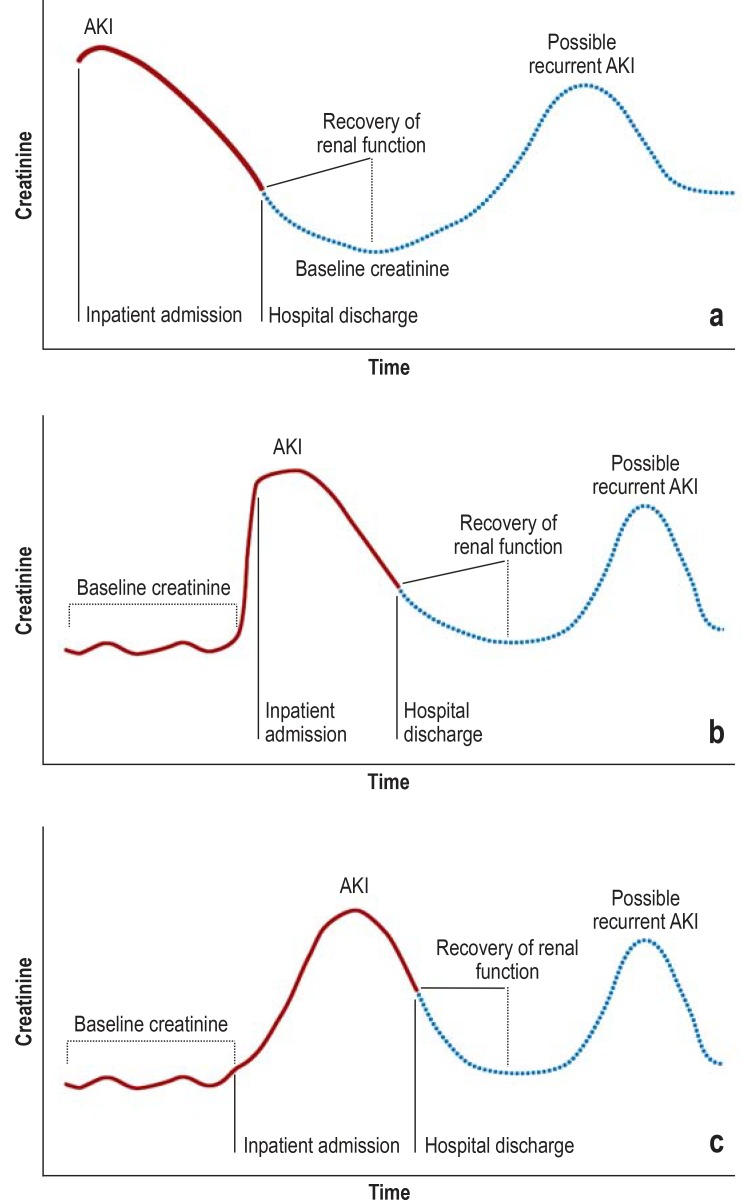
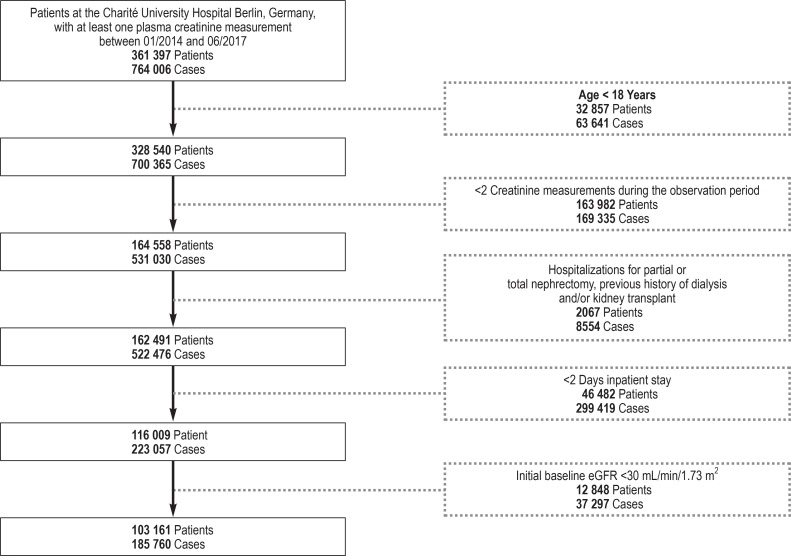
Methods: In an exploratory approach, we retrospectively analyzed all episodes of AKI over a period of 3.5 years (2014-2017) on the basis of routinely obtained serum creatinine measurements in 103 161 patients whose creatinine had been measured at least twice and who had been in the hospital for at least two days. We used the "Kidney Disease: Improving Global Outcomes" (KDIGO) criteria for AKI. In parallel, we assessed the administrative coding of discharge diagnoses of the same patients with codes from the International Classification of Diseases (ICD-10-GM).
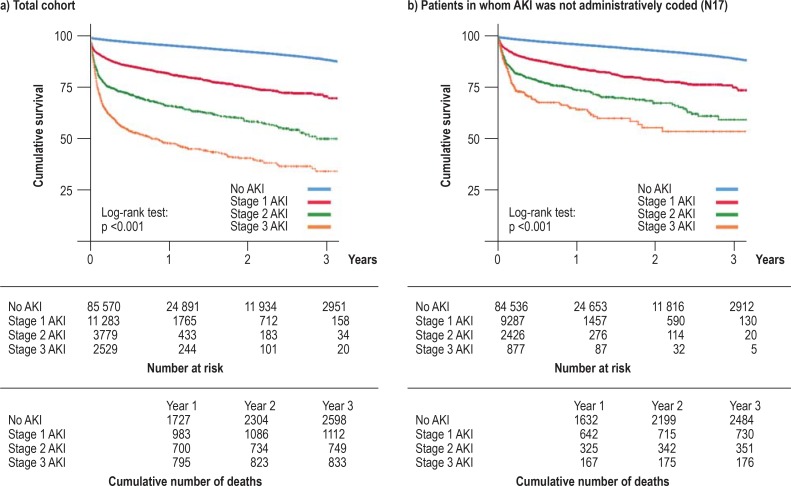
Results: Among 185 760 hospitalizations, stage 1 AKI occurred in 25 417 cases (13.7%), stage 2 in 8503 cases (4.6%), and stage 3 in 5881 cases (3.1%). AKI cases were associated with length of hospital stay, renal morbidity, and overall mortality, and this association was stage-dependent. The in-hospital mortality was 5.1% for patients with stage 1 AKI, 13.7% for patients with stage 2 AKI, and 24.8% for patients with stage 3 AKI. An administrative coding for acute kidney injury (N17) was present in only 28.8% (11 481) of the AKI cases that were identified by creatinine criteria. Like the AKI cases overall, those that were identified by creatinine criteria but were not coded as AKI had significantly higher mortality, and this association was stage-dependent.
Conclusion: AKI episodes are common among hospitalized patients and are associated with considerable morbidity and mortality, yet they are inadequately documented and probably often escape the attention of the treating physicians.
Figures
References
-
- Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol. 2005;16:3365–3370. - PubMed
-
- Chertow GM, Soroko SH, Paganini EP, et al. Mortality after acute renal failure: models for prognostic stratification and risk adjustment. Kidney Int. 2006;70:1120–1126. - PubMed
-
- Liangos O, Wald R, O‘Bell JW, Price L, Pereira BJ, Jaber BL. Epidemiology and outcomes of acute renal failure in hospitalized patients: a national survey. Clin J Am Soc Nephrol. 2006;1:43–51. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources