

Mortality and Medical Comorbidity in the Severely Mentally Ill
- PMID: 31366432
- PMCID: PMC6683445
- DOI: 10.3238/arztebl.2019.0405
Mortality and Medical Comorbidity in the Severely Mentally Ill
Abstract
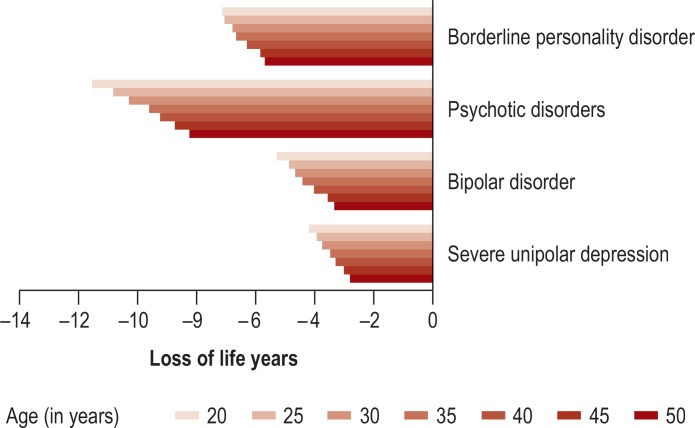
Background: Mentally ill patients die on average 10 years earlier than the general population, largely due to general medical disorders. This study is the first to explore in a large German sample the prevalence, mortality, and medical comorbidity in pa- tients with severe mental illness (SMI). The patients were affected by borderline personality disorder (BPD), psychotic disorders, bipolar disorder, or severe unipolar depression.
Methods: Our database consists of billing data from all adults with statutory health insurance in Germany. Twelve-month administrative SMI prevalence and medical comorbidity were estimated using cross-sectional data from 2016 (age ≥ 18; N = 59 561 310). Two-year mortality was established longitudinally in a randomly selected subset of the billing data (most recent mortality information available for 2012 to 2014; 2012: n = 15 590 107).
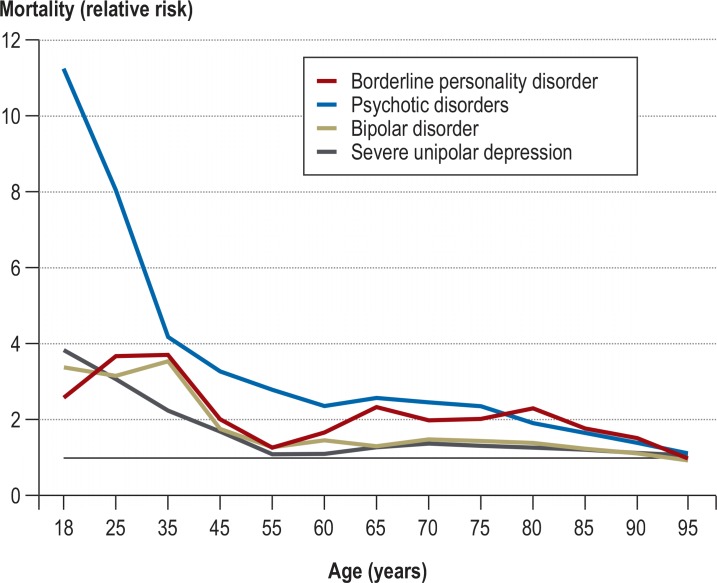
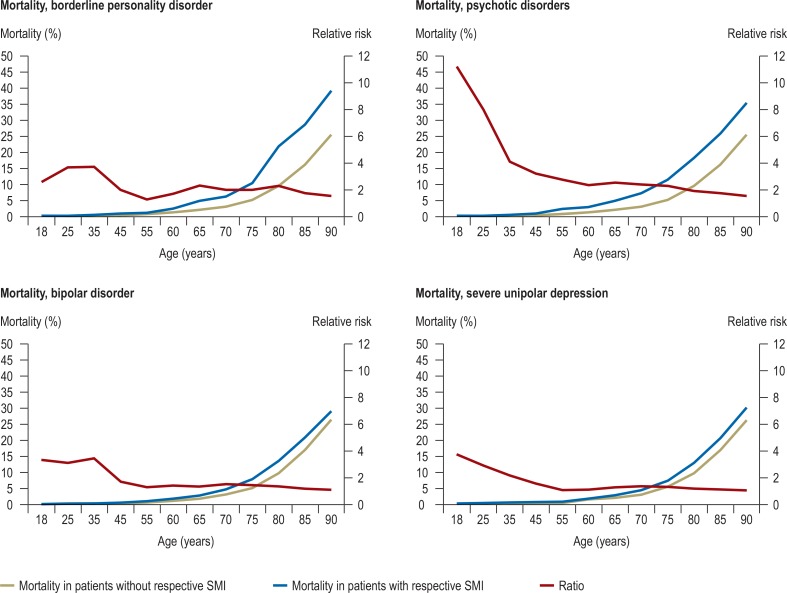
Results: Severe unipolar depression had the highest prevalence (2.01%), followed by psychotic disorders (1.25%), BPD (0.34%), and bipolar disorder (0.29%). While the prevalence of malignant neoplasms showed moderate deviations from reference values [severe unipolar depression: OR = 1.30 (95% CI = 1.29; 1.31), BPD: OR = 1.11 (1.09; 1.14), psychotic dis- orders: OR = 0.90 (0.89; 0.90), bipolar disorder: OR = 1.07 (1.06; 1.09)], other disease groups (infectious, endocrine/nutritional/ metabolic, circulatory, respiratory) were substantially elevated in all categories of SMI. Mortality rates for psychotic disorders, BPD, bipolar disorder, and severe unipolar depression were increased (OR = 2.38 [95% CI=2.32; 2.44], 2.30 [2.08; 2.54], 1.52 [1.42; 1.62], and 1.40 [1.37; 1.44], respectively), with a loss of 2.6 to 12.3 years, depending on age, sex, and SMI.
Conclusion: Mortality is substantially elevated in all SMI patients. The results underline the need to remove barriers to adequate general medical care, both on the patient and the provider side, to reduce excess mortality.
Figures
Comment in
-
Risk of Rehospitalization can be Reduced.Dtsch Arztebl Int. 2019 Oct 11;116(41):689. doi: 10.3238/arztebl.2019.0689a. Dtsch Arztebl Int. 2019. PMID: 31709973 Free PMC article. No abstract available.
-
In Reply.Dtsch Arztebl Int. 2019 Oct 11;116(41):689-690. doi: 10.3238/arztebl.2019.0689b. Dtsch Arztebl Int. 2019. PMID: 31709974 Free PMC article. No abstract available.
References
-
- Wahlbeck K, Westman J, Nordentoft M, Gissler M, Laursen TM. Outcomes of nordic mental health systems: life expectancy of patients with mental disorders. Br J Psychiatry. 2011;199:453–458. - PubMed
-
- Hjorthøj C, Østergaard MLD, Benros ME, et al. Association between alcohol and substance use disorders and all-cause and cause-specific mortality in schizophrenia, bipolar disorder, and unipolar depression: A nationwide, prospective, register-based study. The Lancet Psychiatry. 2015;2:801–808. - PubMed