

Screening for pulmonary arterial hypertension in systemic sclerosis
- PMID: 31366460
- PMCID: PMC9488700
- DOI: 10.1183/16000617.0023-2019
Screening for pulmonary arterial hypertension in systemic sclerosis
Abstract
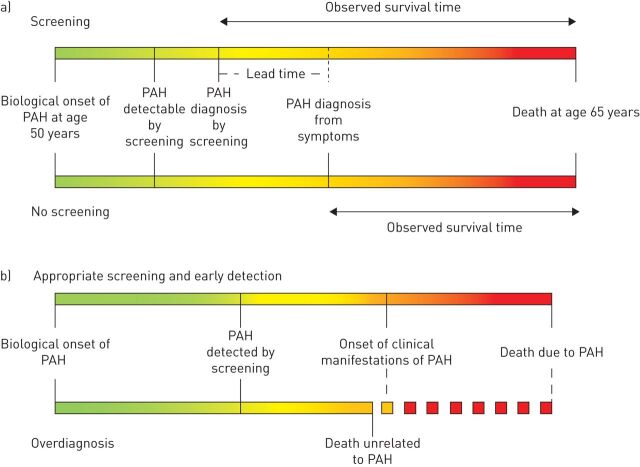
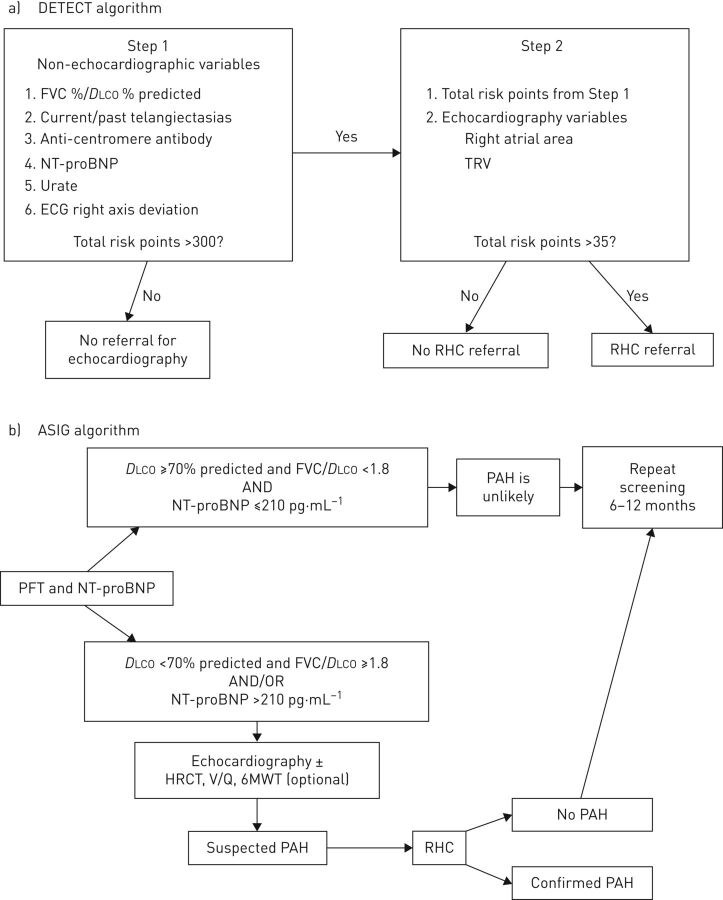
Pulmonary arterial hypertension (PAH) is a dreaded complication of systemic sclerosis (SSc) that occurs in ∼10% of patients. Most individuals present with severe symptoms, significant functional impairment and severe haemodynamics at diagnosis, and survival after PAH diagnosis is poor. Therefore, early diagnosis through systematic screening of asymptomatic patients has the potential to identify PAH at an early stage. Current evidence suggests that early diagnosis and treatment of PAH in patients with SSc may lead to better clinical outcomes. Annual screening may include echocardiography, but this can miss some patients due to suboptimal visualisation or insufficient tricuspid regurgitation. Other options for screening include the DETECT algorithm or the use of a combination of pulmonary function testing (forced vital capacity/diffusing capacity of the lung for carbon monoxide ratio) and N-terminal-pro-brain natriuretic peptide levels. Symptomatic patients, those with an elevated tricuspid regurgitation velocity on echocardiogram with or without secondary echocardiographic features of PAH, and those who screen positive on the DETECT or other pulmonary function test algorithms should undergo right heart catheterisation. Exercise echocardiography or cardiopulmonary exercise testing, nailfold capillaroscopy and molecular biomarkers are promising but, as yet, unproven potential options. Future screening studies should employ systematic catheterisation to define the true predictive values for PAH.
Copyright ©ERS 2019.
Conflict of interest statement
Conflict of interest: J. Weatherald reports grants, personal fees and non-financial support from Actelion, personal fees and non-financial support from Bayer, personal fees from Novartis, and grants from the European Respiratory Society and Canadian Vascular Network, outside the submitted work. Conflict of interest: D. Montani reports grants and personal fees from Actelion and Bayer, and personal fees from GSK, MSD and Pfizer, outside the submitted work. Conflict of interest: M. Jevnikar has nothing to disclose. Conflict of interest: X. Jais reports grants, personal fees and non-financial support from Actelion and Bayer, personal fees and non-financial support from MSD, and grants and non-financial support from GSK, outside the submitted work. Conflict of interest: L. Savale reports grants, personal fees and non-financial support from Actelion, Bayer, MSD and GSK, outside the submitted work. Conflict of interest: M. Humbert reports personal fees and non-financial support from Actelion, grants, personal fees and non-financial support from Bayer, grants and personal fees from GSK, and personal fees from Merck and United Therapeutics, outside the submitted work.
Figures
References
-
- Galiè N, Humbert M, Vachiery J-L, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Respir J 2015; 46: 903–975. - PubMed
-
- Kovacs G, Berghold A, Scheidl S, et al. Pulmonary arterial pressure during rest and exercise in healthy subjects: a systematic review. Eur Respir J 2009; 34: 888–894. - PubMed
-
- Humbert M, Sitbon O, Chaouat A, et al. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med 2006; 173: 1023–1030. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical