

Gastrointestinal Stromal Tumor (GIST) from esophagus to anorectum - diagnosis, response evaluation and surveillance on computed tomography (CT) scan
- PMID: 31367084
- PMCID: PMC6639866
- DOI: 10.4103/ijri.IJRI_354_18
Gastrointestinal Stromal Tumor (GIST) from esophagus to anorectum - diagnosis, response evaluation and surveillance on computed tomography (CT) scan
Abstract
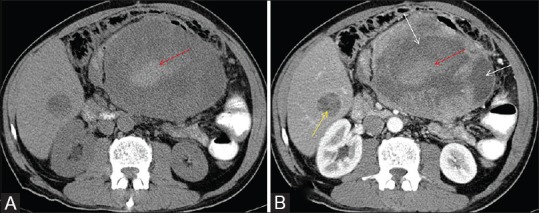
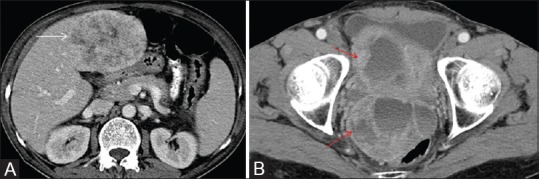
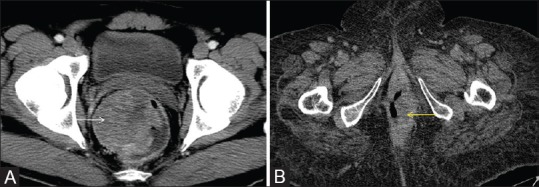
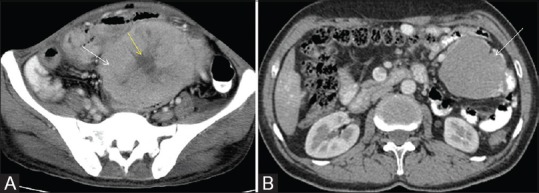
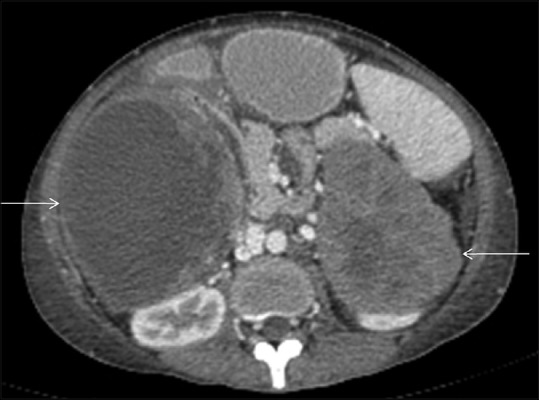
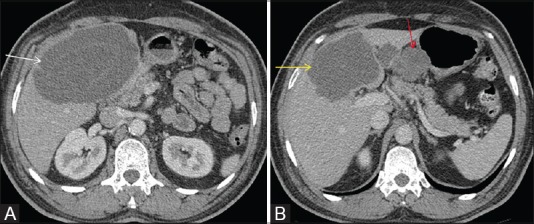
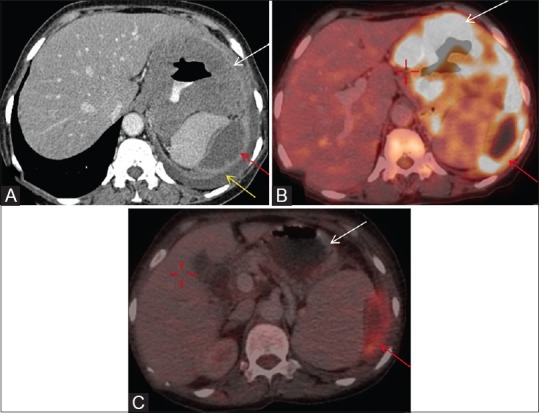
Gastrointestinal stromal tumor (GIST) are the most common non epithelial tumor of the gastrointestinal (GI) tract. They arise from interstitial cells of Cajal present in the myenteric plexus. They can also arise outside the GI tract from mesentery, retro peritoneum and omentum. With the advent of new targeted molecular therapy c- tyrosine kinase inhibitor (Imatinib), it has become important to differentiate between response and pseudo-progression of the disease as response evaluation criteria for GIST are different from Response Evaluation Criteria in Solid Tumors (RECIST). Purpose of this pictorial essay is to enumerate the characteristic CT features of GIST, and discuss atypical features and response evaluation criteria.
Keywords: GIST; gastrointestinal; imatinib; tumor.
Conflict of interest statement
There are no conflicts of interest.
Figures



References
-
- Lakshmi VA, Chacko RT, Kurian S. Gastrointestinal stromal tumors: A 7-year experience from a tertiary care hospital. Indian J Pathol Microbiol. 2010;53:628–33. - PubMed
-
- Joensuu H, Fletcher C, Dimitrijevic S, Silberman S, Roberts P, Demetri G. Management of malignant gastrointestinal stromal tumours. Lancet Oncol. 2002;3:655–64. - PubMed
-
- Rubin BP, Heinrich MC, Corless CL. Gastrointestinal stromal tumour. Lancet. 2007;19(369):1731–41. - PubMed
-
- Steigen SE, Eide TJ. Gastrointestinal stromal tumors (GISTs): A review. APMIS. 2009;12(117):73–86. - PubMed
-
- Nishida T, Hirota S. Biological and clinical review of stromal tumors in the gastrointestinal tract. Histol Histopathol. 2000;15:1293–301. - PubMed