

Barium esophagogram in various esophageal diseases: A pictorial essay
- PMID: 31367085
- PMCID: PMC6639862
- DOI: 10.4103/ijri.IJRI_465_18
Barium esophagogram in various esophageal diseases: A pictorial essay
Abstract
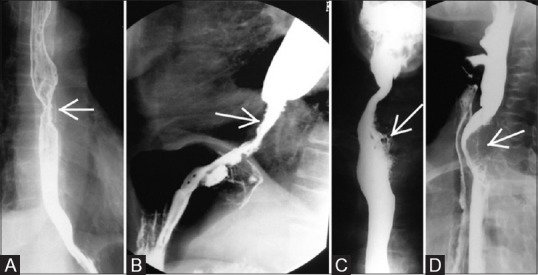
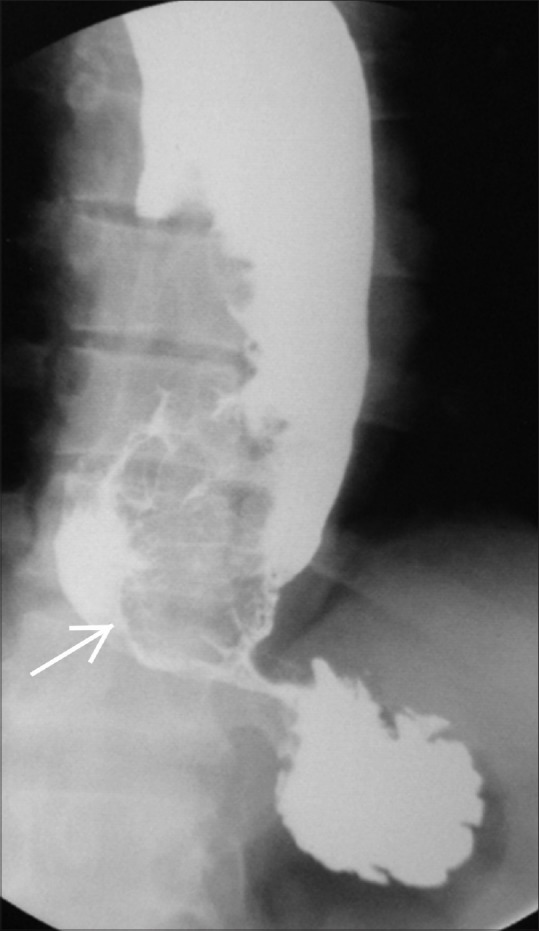
Recent years have seen a decline in number of barium procedures due to wider availability of cross sectional imaging modalities. Though use of barium esophagography/barium swallow has decreased in day to day clinical practice, it still remains a valuable test for structural and functional evaluation of esophagus. It can be performed as single or double contrast examination or as a multiphasic examination comprising upright double contrast views followed by prone single contrast views. This pictorial essay demonstrates imaging features of various esophageal diseases on barium esophagogram.
Keywords: Barium swallow; diverticula; esophagus; motility disorder; tumours; webs.
Conflict of interest statement
There are no conflicts of interest.
Figures























References
-
- Rubesin SE. Structural abnormalities of the pharynx. In: Gore RM, Levine MS, editors. Textbook of Gastrointestinal Radiology. 3rd ed. Philadelphia, Pa: Saunders; 2008. pp. 271–308.
-
- Shauffer IA, Phillips HE, Sequeira J. The jet phenomenon a manifestation of esophageal web. AJR. 1977;129:747–8. - PubMed
-
- Taylor AI, Stewart ET, Dodds WJ. The eophageal jet phenomenon revisited. AJR. 1990;155:289–90. - PubMed
-
- Schatzki R. The lower esophageal ring: Long term follow-up of symptomatic and asymptomatic rings. Am J Roentgenol Ra-dium Ther Nucl Med. 1963;90:805–10. - PubMed
-
- Levine MS. Miscellaneous abnormalities of the esophagus. In: Gore RM, Levine MS, editors. Textbook of Gastrointestinal Radiology. 3rd ed. Philadelphia, Pa: Saunders; 2000. pp. 465–93.