

Conventional and magnetic resonance hysterosalpingography in assessing tubal patency-A comparative study
- PMID: 31367087
- PMCID: PMC6639856
- DOI: 10.4103/ijri.IJRI_109_18
Conventional and magnetic resonance hysterosalpingography in assessing tubal patency-A comparative study
Abstract
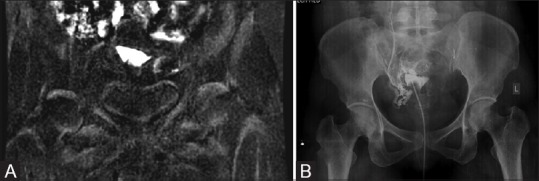
Context: Tubal factors, one of the leading causes of female infertility, have been conventionally evaluated by hysterosalpingography (HSG). The role of magnetic resonance imaging (MRI) in assessing female infertility is gaining importance because of its inherent efficiency in detecting structural abnormalities. Magnetic resonance hysterosalpingography (MR HSG) is less invasive and avoids exposure of ovaries to ionizing radiation. Its utility is extrapolated to visualize fallopian tubes.
Aims: To assess the diagnostic accuracies of dynamic MR HSG and conventional HSG (cHSG) in identifying tubal patency in women with infertility using diagnostic laparoscopy (DL) as gold standard.
Materials and methods: A prospective study of 40 patients was conducted over a period of 6 months. The patients were subjected to MR HSG followed by cHSG during the preovulatory period. If tubes were blocked, the patients were subjected to DL in the next menstrual cycle. If the tubes were patent and there was failure of conception, they were subjected to DL in the interval of 3 months.
Results: Twenty-four patients had bilateral tubal spill which was confirmed using cHSG and DL. One patient had discordant MR HSG and cHSG results and six patients had discordant MR HSG and DL results. No statistical difference was observed between MR HSG and cHSG.
Conclusion: Pelvic MRI is an inevitable tool in infertility evaluation. MR HSG can be used in addition as it avoids exposure of the reproductive organs to radiation and has the same efficacy as cHSG.
Keywords: Conventional hysterosalpingography; diagnostic laparoscopy; female infertility; magnetic resonance hysterosalpingography; tubal patency.
Conflict of interest statement
There are no conflicts of interest.
Figures




Similar articles
-
Fallopian tubal patency diagnosed by magnetic resonance hysterosalpingography.J Reprod Med. 2012 Sep-Oct;57(9-10):435-40. J Reprod Med. 2012. PMID: 23091993
-
Comparison between magnetic resonance hysterosalpingography and conventional hysterosalpingography: direct visualization of the fallopian tubes using a novel MRI contrast agent mixture.Acta Radiol. 2020 Jul;61(7):1001-1007. doi: 10.1177/0284185119883712. Epub 2019 Nov 4. Acta Radiol. 2020. PMID: 31684746
-
Magnetic resonance hysterosalpingography in diagnostic work-up of female infertility - comparison with conventional hysterosalpingography: a randomised study.Eur Radiol. 2019 Feb;29(2):501-508. doi: 10.1007/s00330-018-5572-2. Epub 2018 Jul 4. Eur Radiol. 2019. PMID: 29974219 Clinical Trial.
-
Hysterosalpingo-contrast-sonography vs. magnetic resonance-hysterosalpingography for diagnosing fallopian tubal patency: A systematic review and meta-analysis.Eur J Radiol. 2020 Apr;125:108891. doi: 10.1016/j.ejrad.2020.108891. Epub 2020 Feb 20. Eur J Radiol. 2020. PMID: 32088657
-
Hysterosalpingography using Magnetic Resonance Imaging for infertility patients.JBRA Assist Reprod. 2021 Jul 21;25(3):403-411. doi: 10.5935/1518-0557.20210002. JBRA Assist Reprod. 2021. PMID: 33900058 Free PMC article. Review.
Cited by
-
Evaluation of tubal patency based on peak injection pressure in four-dimensional hysterosalpingo-contrast sonography among infertile females: a preliminary study.Quant Imaging Med Surg. 2024 May 1;14(5):3461-3472. doi: 10.21037/qims-23-1569. Epub 2024 Apr 26. Quant Imaging Med Surg. 2024. PMID: 38720834 Free PMC article.
-
Diagnostic accuracy of pelvis multiparametric MRI against CT virtual hysterosalpingography: a prospective study of tubal patency through female infertility assessment.Br J Radiol. 2023 Jun 1;96(1146):20220889. doi: 10.1259/bjr.20220889. Epub 2023 Apr 22. Br J Radiol. 2023. PMID: 37066809 Free PMC article.
References
-
- Zegers-Hochschild F, Adamson GD, de Mouzon J, Ishihara O, Mansour R, Nygren K, et al. The international committee for monitoring assisted reproductive technology (ICMART) and the world health organization (WHO) revised glossary on ART terminology, human reproduction. 2009;24:2683–7. - PubMed
-
- Steinkeler JA, Woodfield CA, Lazarus E, Hillstrom MM. Female infertility: A systematic approach to radiologic imaging and diagnosis. Radiographics. 2009;29:1353–70. - PubMed
-
- Simpson Jr WL, Beitia LG, Mester J. Hysterosalpingography: A reemerging study. Radiographics. 2006;26:419–31. - PubMed
-
- Sadowski EA, Ochsner JE, Riherd JM, Korosec FR, Agrawal G, Pritts EA, et al. MR hysterosalpingography with an angiographic time-resolved 3D pulse sequence: Assessment of tubal patency. AJR Am J Roentgenol. 2008;191:1381–5. - PubMed