

Real-time PCR and targeted next-generation sequencing in the detection of low level EGFR mutations: Instructive case analyses
- PMID: 31367517
- PMCID: PMC6656700
- DOI: 10.1016/j.rmcr.2019.100901
Real-time PCR and targeted next-generation sequencing in the detection of low level EGFR mutations: Instructive case analyses
Abstract
Background: Allele specific real-time PCR and next-generation sequencing (NGS) are widely used to detect somatic mutation in non-small cell lung cancer (NSCLC). Both methods commonly use formalin-fixed paraffin-embedded (FFPE) tissues as diagnostic materials. Real-time PCR has the advantage of being easy to use and more tolerant of variable DNA quality, but has limited multiplex capability. NGS, in contrast, allows simultaneous analysis of many genomic loci while revealing the exact sequence changes; it is, however, more technically demanding and more expensive to employed. A challenge for both platforms is the varied limit of detection (LoD) for target genomic loci, even within the same gene. The variability of detection sensitivity may be problematic if well-known actionable somatic mutations are missed.
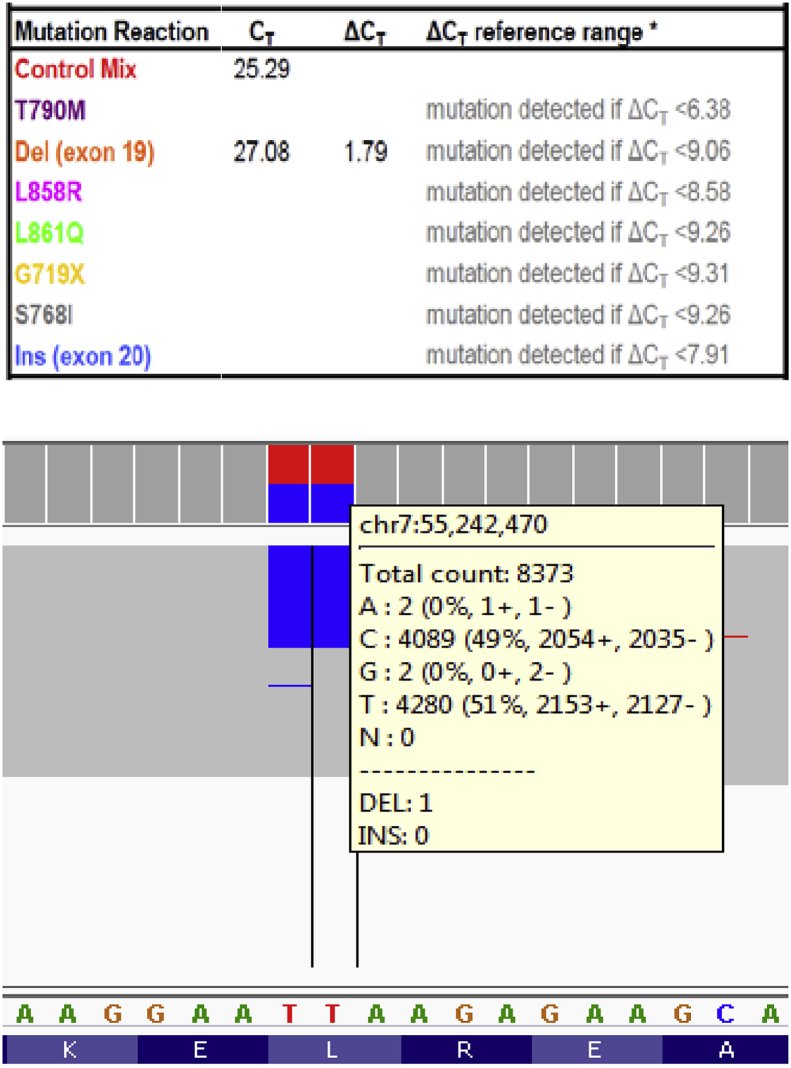
Cases: We compared LoDs between real-time PCR and targeted NGS tests for some commonly observed EGFR mutations in NSCLC specimens.
Conclusions: The FDA-approved real-time PCR test was superior to the NGS in detecting low level EGFR exon 19 deletion (near 1% variant allele fraction (VAF)). The cancer hotspot NGS detects low level EGFR c.2369C > T, p.T790M (2-5% VAF) better than the FDA-approved real-time PCR method. We conclude that the real-time PCR and hotspot NGS methods have complementary strengths in accurately determining clinically important EGFR mutations in NSCLC.
Keywords: Epidermal growth factor receptor; FDA; Fine needle aspiration; Formalin-fixed paraffin-embedded tissue; Next-generation sequencing; Non-small cell lung cancer; therascreen®.
Figures
References
-
- Siegel R.L., Miller K.D., Jemal A. Cancer statistics. Ca - Cancer J. Clin. 2015;65(1):5–29. http://www.ncbi.nlm.nih.gov/pubmed/25559415 2015. - PubMed
-
- Doxtader E.E., Cheng Y.W., Zhang Y. Molecular testing of non-small cell lung carcinoma diagnosed by endobronchial ultrasound-guided transbronchial fine-needle aspiration. Arch. Pathol. Lab Med. 2019;143(6):670–676. http://www.ncbi.nlm.nih.gov/pubmed/29372844 - PubMed
-
- Lynch T.J., Bell D.W., Sordella R., Gurubhagavatula S., Okimoto R.A., Brannigan B.W., Harris P.L., Haserlat S.M., Supko J.G., Haluska F.G., Louis D.N., Christiani D.C., Settleman J., Haber D.A. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N. Engl. J. Med. 2004;350(21):2129–2139. http://www.ncbi.nlm.nih.gov/pubmed/15118073 - PubMed
-
- Paez J.G., Janne P.A., Lee J.C., Tracy S., Greulich H., Gabriel S., Herman P., Kaye F.J., Lindeman N., Boggon T.J., Naoki K., Sasaki H., Fujii Y., Eck M.J., Sellers W.R., Johnson B.E., Meyerson M. EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science. 2004;304(5676):1497–1500. http://www.ncbi.nlm.nih.gov/pubmed/15118125 - PubMed
-
- Pao W., Miller V., Zakowski M., Doherty J., Politi K., Sarkaria I., Singh B., Heelan R., Rusch V., Fulton L., Mardis E., Kupfer D., Wilson R., Kris M., Varmus H. EGF receptor gene mutations are common in lung cancers from "never smokers" and are associated with sensitivity of tumors to gefitinib and erlotinib. Proc. Natl. Acad. Sci. U. S. A. 2004;101(36):13306–13311. http://www.ncbi.nlm.nih.gov/pubmed/15329413 - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
