

PLA2R-Negative Membranous Nephropathy Presenting as a Prodrome of IgG4-Related Autoimmune Pancreatitis
- PMID: 31367609
- PMCID: PMC6616050
- DOI: 10.1159/000501260
PLA2R-Negative Membranous Nephropathy Presenting as a Prodrome of IgG4-Related Autoimmune Pancreatitis
Abstract
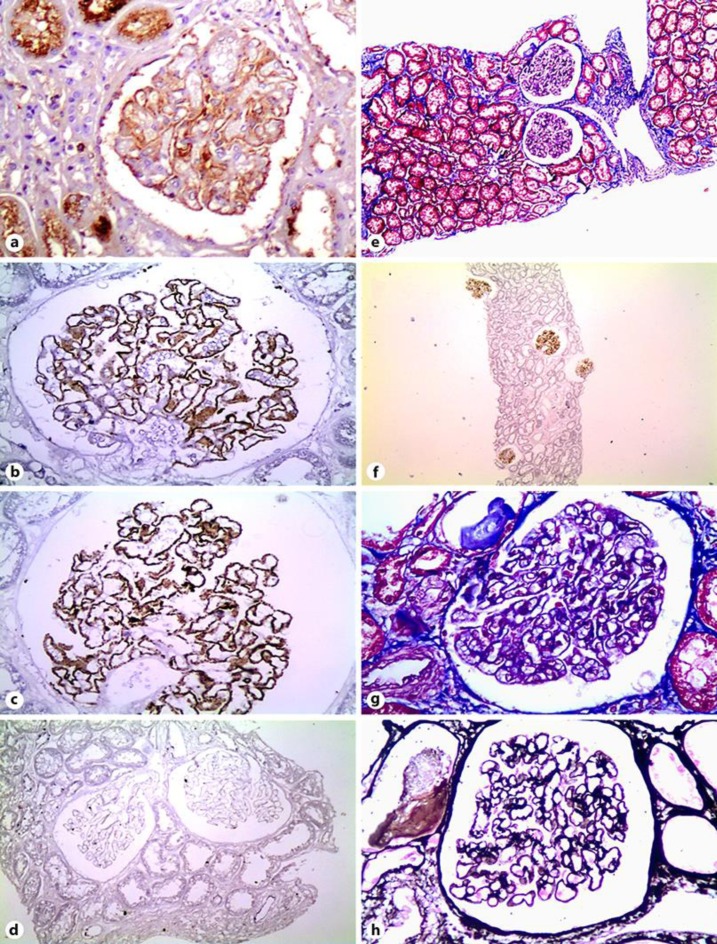
Membranous nephropathy (MN) with tubulointerstitial nephritis (TIN) is an established manifestation of immunoglobulin G4 (IgG4)-related disease (IgG4-RD). A pathological feature aiming to distinguish between primary and secondary MN is the presence or absence of glomerular staining for phospholipase A2 receptor (PLA2R), respectively. Isolated MN without TIN has been rarely reported in the context of IgG4-RD. This case report describes a patient with a history of MN successfully treated with steroids and cyclophosphamide, who, 3 years later, presented with unexplained exacerbation of diabetes mellitus due to IgG4-related autoimmune pancreatitis. Pancreatitis was treated, and diabetes improved after treatment with steroids. Based on the presence of isolated IgG4 glomerular capillary deposits along with negative staining for PLA2R and the metachronous appearance of autoimmune pancreatitis, MN was retrospectively classified as secondary to IgG4-RD. Isolated IgG4-positive/PLA2R-negative MN without TIN can be a prodrome of IgG4-RD, reminiscent of MN secondary to neoplasms.
Keywords: Autoimmune pancreatitis; Diabetes mellitus; Endoscopic ultrasound; IgG4-related disease; Membranous nephropathy; PLA2R.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
A case of PLA2R-positive membranous nephropathy with subsequent development of IgG4-related disease.CEN Case Rep. 2025 Apr;14(2):280-290. doi: 10.1007/s13730-024-00941-8. Epub 2024 Nov 8. CEN Case Rep. 2025. PMID: 39514162 Free PMC article.
-
IgG4-related disease complicated by PLA2R-associated membranous nephropathy: A case report.Open Life Sci. 2024 Jul 25;19(1):20220921. doi: 10.1515/biol-2022-0921. eCollection 2024. Open Life Sci. 2024. PMID: 39071497 Free PMC article.
-
Phospholipase A2 receptor-associated membranous nephropathy in a patient with IgG4-related disease: A case report.Medicine (Baltimore). 2019 May;98(20):e15616. doi: 10.1097/MD.0000000000015616. Medicine (Baltimore). 2019. PMID: 31096469 Free PMC article.
-
IgG4-related kidney disease (IgG4-RKD) with membranous nephropathy as its initial manifestation: report of one case and literature review.BMC Nephrol. 2019 Jul 16;20(1):263. doi: 10.1186/s12882-019-1419-6. BMC Nephrol. 2019. PMID: 31311519 Free PMC article. Review.
-
Immunology of membranous nephropathy: from animal models to humans.Clin Exp Immunol. 2016 Feb;183(2):157-65. doi: 10.1111/cei.12729. Epub 2015 Nov 24. Clin Exp Immunol. 2016. PMID: 26459770 Free PMC article. Review.
Cited by
-
A case of PLA2R-positive membranous nephropathy with subsequent development of IgG4-related disease.CEN Case Rep. 2025 Apr;14(2):280-290. doi: 10.1007/s13730-024-00941-8. Epub 2024 Nov 8. CEN Case Rep. 2025. PMID: 39514162 Free PMC article.
References
-
- Fragoulis GE, Moutsopoulos HM. IgG4 syndrome: old disease, new perspective. J Rheumatol. 2010 Jul;37((7)):1369–70. - PubMed
-
- Mahajan VS, Mattoo H, Deshpande V, Pillai SS, Stone JH. IgG4-related disease. Annu Rev Pathol. 2014;9((1)):315–47. - PubMed
-
- Deshpande V, Zen Y, Chan JK, Yi EE, Sato Y, Yoshino T, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. 2012 Sep;25((9)):1181–92. - PubMed
-
- Finkelberg DL, Sahani D, Deshpande V, Brugge WR. Autoimmune pancreatitis. N Engl J Med. 2006 Dec;355((25)):2670–6. - PubMed
-
- Chari ST, Takahashi N, Levy MJ, Smyrk TC, Clain JE, Pearson RK, et al. A diagnostic strategy to distinguish autoimmune pancreatitis from pancreatic cancer. Clin Gastroenterol Hepatol. 2009 Oct;7((10)):1097–103. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
