

The relative efficiency of time-to-progression and continuous measures of cognition in presymptomatic Alzheimer's disease
- PMID: 31367671
- PMCID: PMC6656701
- DOI: 10.1016/j.trci.2019.04.004
The relative efficiency of time-to-progression and continuous measures of cognition in presymptomatic Alzheimer's disease
Abstract
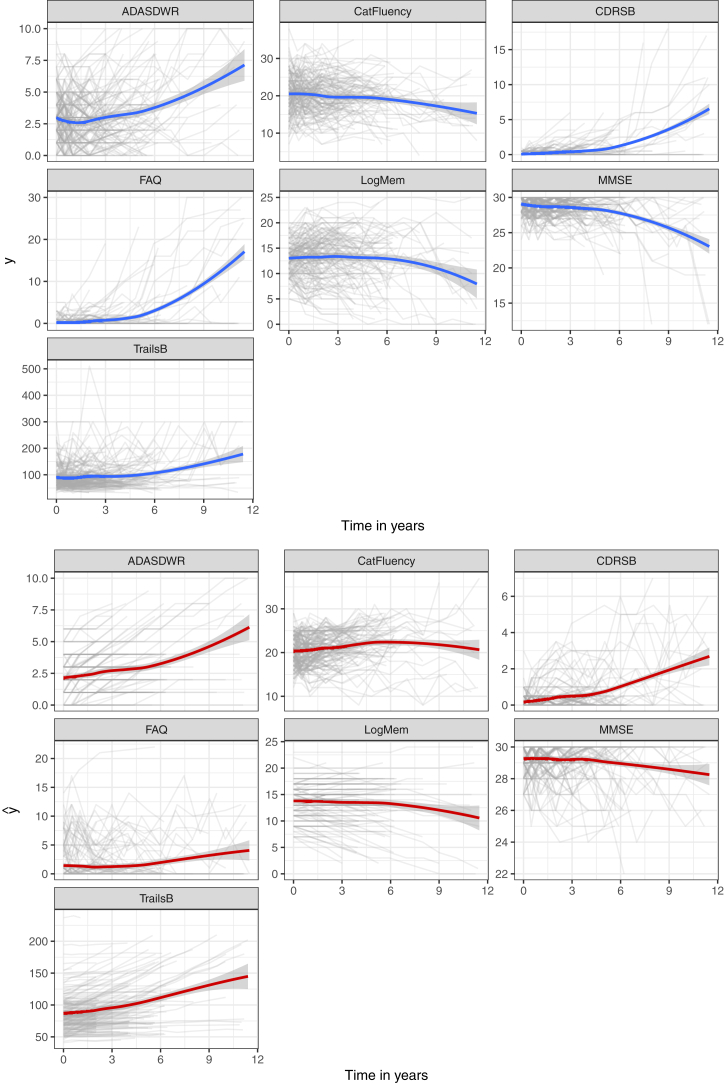
Introduction: Clinical trials on preclinical Alzheimer's disease are challenging because of the slow rate of disease progression. We use a simulation study to demonstrate that models of repeated cognitive assessments detect treatment effects more efficiently than models of time to progression.
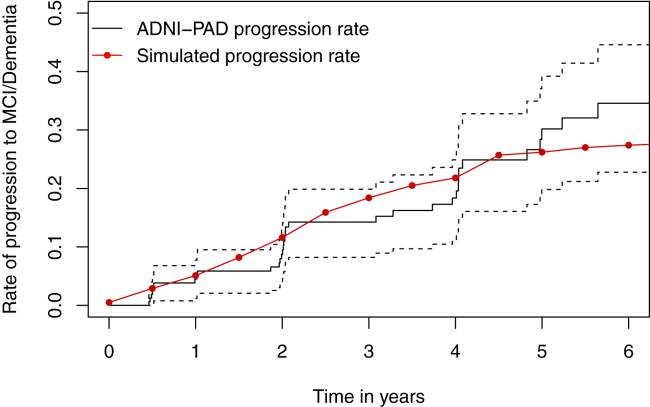
Methods: Multivariate continuous data are simulated from a Bayesian joint mixed-effects model fit to data from the Alzheimer's Disease Neuroimaging Initiative. Simulated progression events are algorithmically derived from the continuous assessments using a random forest model fit to the same data.
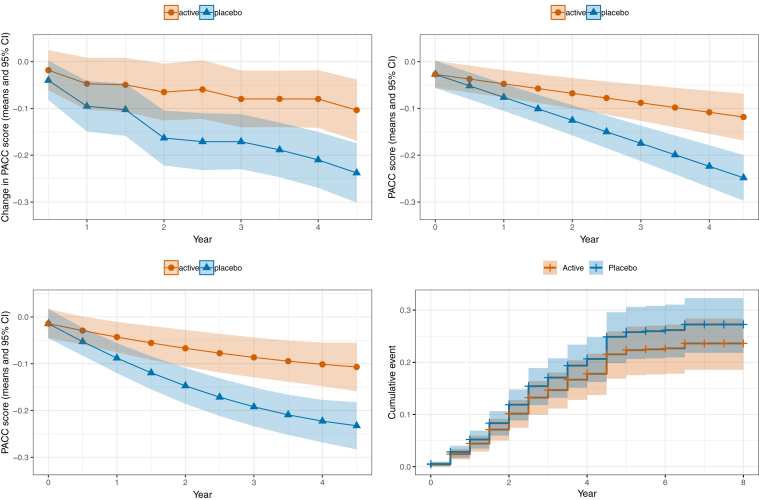
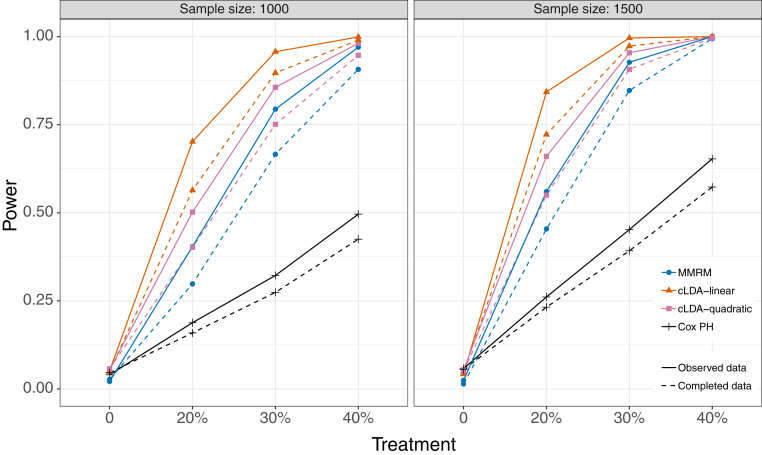
Results: We find that power is approximately doubled with models of repeated continuous outcomes compared with the time-to-progression analysis. The simulations also demonstrate that a plausible informative missing data pattern can induce a bias that inflates treatment effects, yet 5% type I error is maintained.
Discussion: Given the relative inefficiency of time to progression, it should be avoided as a primary analysis approach in clinical trials of preclinical Alzheimer's disease.
Keywords: Alzheimer's disease; Bayesian joint mixed-effect model; Clinical trial simulations; Common close design; Cox proportional hazards model; Longitudinal data; Mixed model of repeated measures (MMRM); Statistical power.
Figures
References
-
- Sperling R.A., Aisen P.S., Beckett L.A., Bennett D.A., Craft S., Fagan A.M. Toward defining the preclinical stages of Alzheimer's disease: Recommendations from the National Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimer's Demen. 2011;7:280–292. - PMC - PubMed
-
- ClinicalTrials.gov An efficacy and safety study of atabecestat in participants who are asymptomatic at risk for developing Alzheimer's dementia (EARLY), Tech. rep., National Library of Medicine (US), Bethesda, MD (2015 Oct 6 - 2019 Jan 21) https://clinicaltrials.gov/ct2/show/NCT02569398 Accessed January 2019.
-
- Caputo A., Racine A., Paule I., Martens E.P., Tariot P., Langbaum J.B. Rationale for selection of primary endpoints in the Alzheimer Prevention Initiative Generation study in cognitively healthy APOE4 homozygotes, Alzheimer's & Dementia. J Alzheimer's Assoc. 2017;13:P1452.