

Rapid breath analysis for acute respiratory distress syndrome diagnostics using a portable two-dimensional gas chromatography device
- PMID: 31367803
- PMCID: PMC6722019
- DOI: 10.1007/s00216-019-02024-5
Rapid breath analysis for acute respiratory distress syndrome diagnostics using a portable two-dimensional gas chromatography device
Abstract
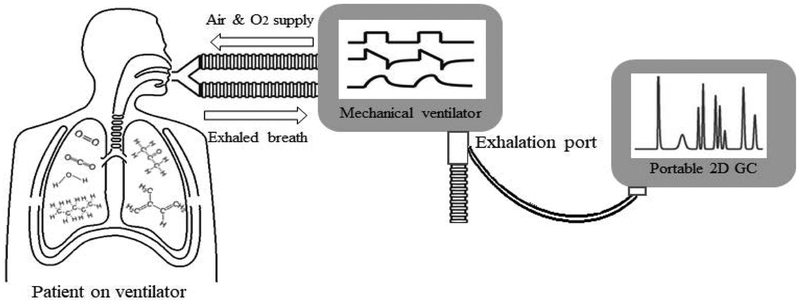
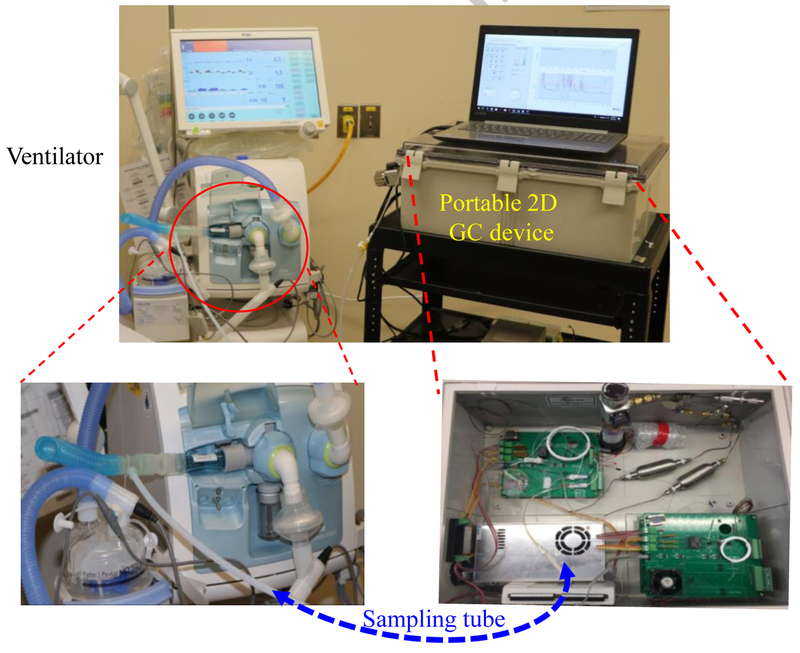
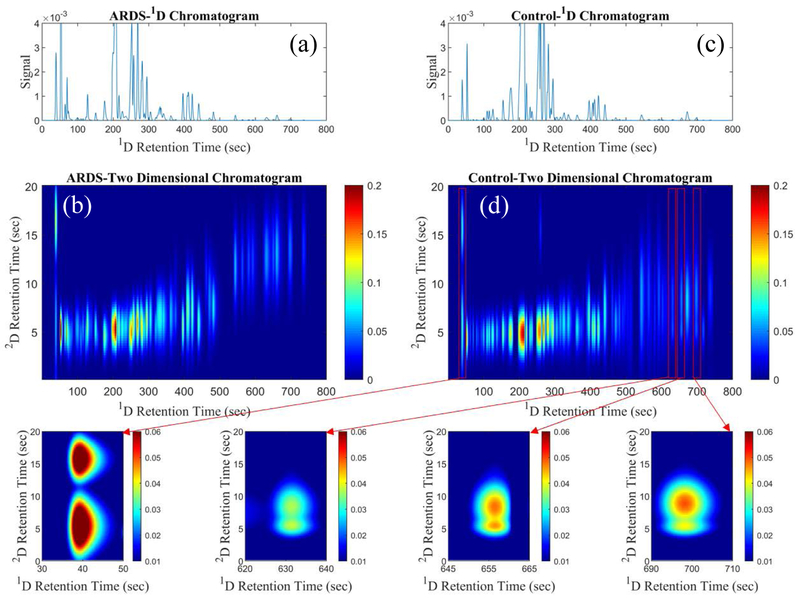
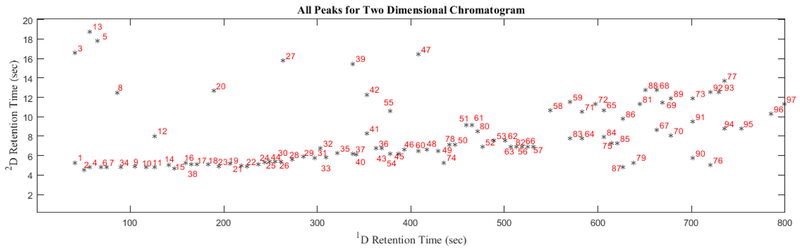
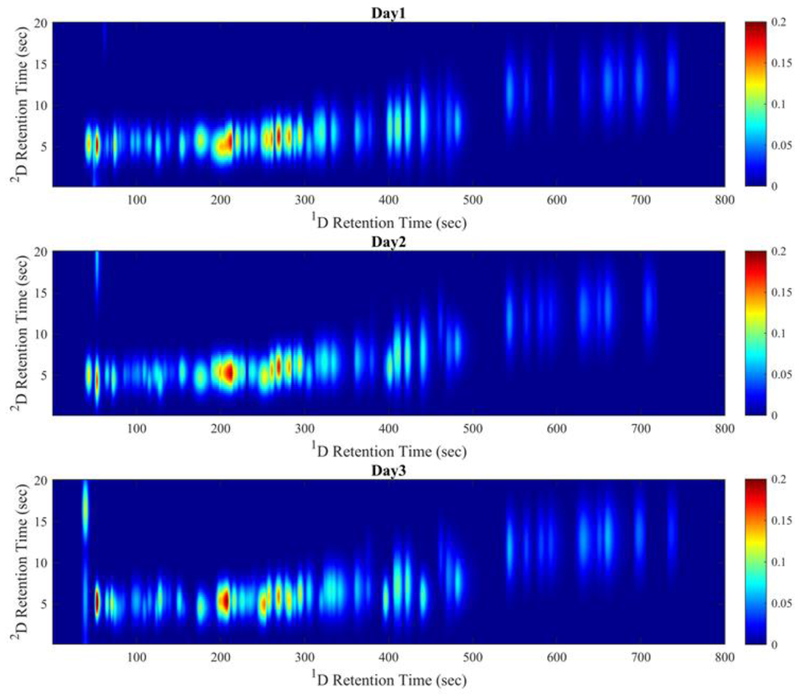
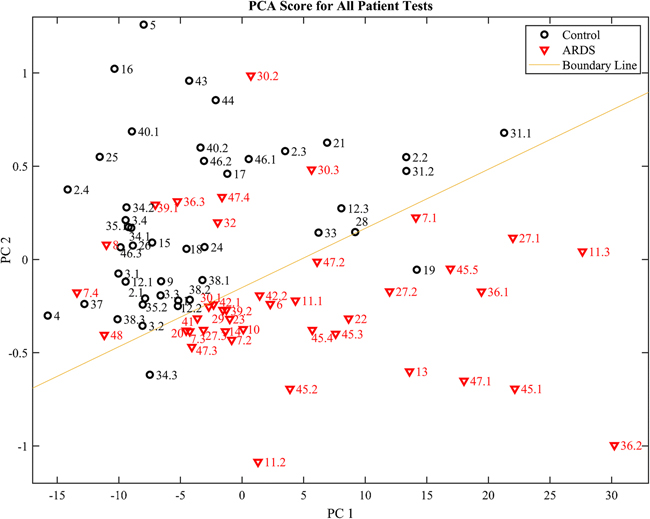
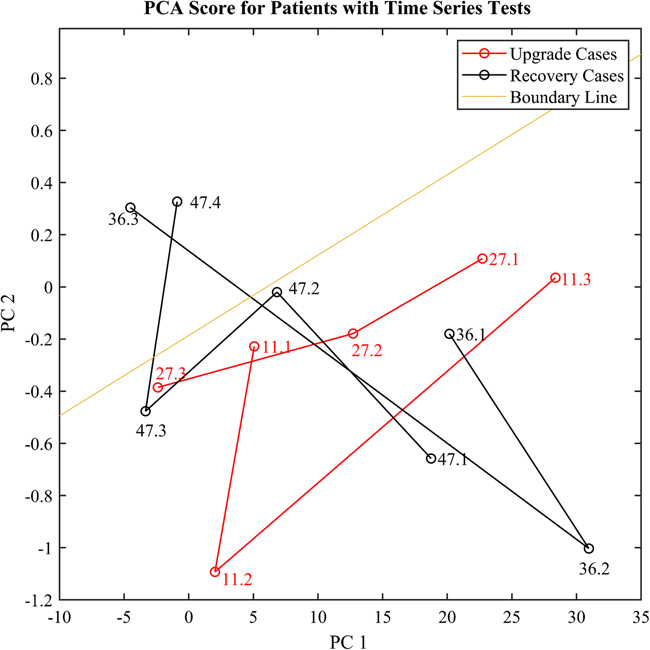
Acute respiratory distress syndrome (ARDS) is the most severe form of acute lung injury, responsible for high mortality and long-term morbidity. As a dynamic syndrome with multiple etiologies, its timely diagnosis is difficult as is tracking the course of the syndrome. Therefore, there is a significant need for early, rapid detection and diagnosis as well as clinical trajectory monitoring of ARDS. Here, we report our work on using human breath to differentiate ARDS and non-ARDS causes of respiratory failure. A fully automated portable 2-dimensional gas chromatography device with high peak capacity (> 200 at the resolution of 1), high sensitivity (sub-ppb), and rapid analysis capability (~ 30 min) was designed and made in-house for on-site analysis of patients' breath. A total of 85 breath samples from 48 ARDS patients and controls were collected. Ninety-seven elution peaks were separated and detected in 13 min. An algorithm based on machine learning, principal component analysis (PCA), and linear discriminant analysis (LDA) was developed. As compared to the adjudications done by physicians based on the Berlin criteria, our device and algorithm achieved an overall accuracy of 87.1% with 94.1% positive predictive value and 82.4% negative predictive value. The high overall accuracy and high positive predicative value suggest that the breath analysis method can accurately diagnose ARDS. The ability to continuously and non-invasively monitor exhaled breath for early diagnosis, disease trajectory tracking, and outcome prediction monitoring of ARDS may have a significant impact on changing practice and improving patient outcomes. Graphical abstract.
Keywords: 2D GC; Acute respiratory distress syndrome gas chromatography; Breath analysis; Machine learning.
Conflict of interest statement
Conflict of interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
Figures
References
-
- Rubenfeld GD, Caldwell E, Peabody E, Weaver J, Martin DP, Neff M, Stern EJ, Hudson LD. Incidence and outcomes of acute lung injury. N Engl J Med. 2005;353(16):1685–93. - PubMed
-
- Zambon M, Vincent J. L. Mortality rates for patients with acute lung injury/ARDS have decreased over time. Chest. 2008;133(5):1120–7. - PubMed
-
- Crader KM, Repine JJD, Repine JE. Breath Biomarkers and the Acute Respiratory Distress Syndrome J Pulmonar Respirat Med. 2012;2(1):111.
-
- Herridge MS, Tansey CM, Matte A, Tomlinson G, Diaz-Granados N, Cooper A, Guest CB, Mazer CD, Mehta S, Stewart TE, Kudlow P, Cook D, Slutsky AS, Cheung AM. Functional disability 5 years after acute respiratory distress syndrome. N Engl J Med. 2011;364(14):1293–304. - PubMed
-
- Mikkelsen ME, Christie JD, Lanken PN, Biester RC, Thompson BT, Bellamy SL, Localio AR, Demissie E, Hopkins RO, Angus DC. The adult respiratory distress syndrome cognitive outcomes study: long-term neuropsychological function in survivors of acute lung injury. Am J Respir Crit Care Med. 2012;185(12):1307–15. - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
