

Safety and effectiveness of ultrasound-guided percutaneous transhepatic biliary drainage: a multicenter experience
- PMID: 31368040
- PMCID: PMC6838250
- DOI: 10.1007/s40477-019-00399-w
Safety and effectiveness of ultrasound-guided percutaneous transhepatic biliary drainage: a multicenter experience
Abstract
Aims: Aim of this study is to describe a multicenter experience on percutaneous transhepatic biliary drainage (PTBD) performed with ultrasound-guidance to access the biliary tree, focusing on safety, effectiveness and radiation dose exposure; differences between right- and left-sided approaches have been also evaluated.
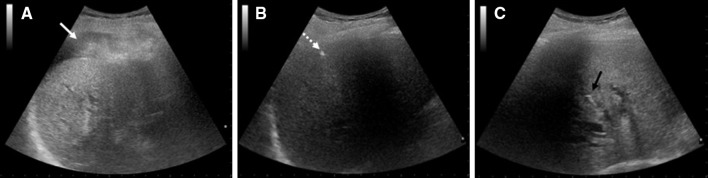
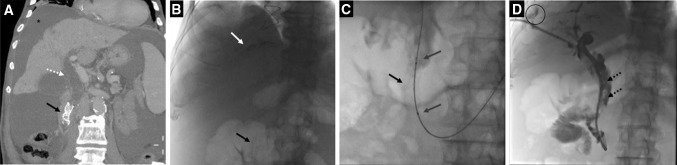
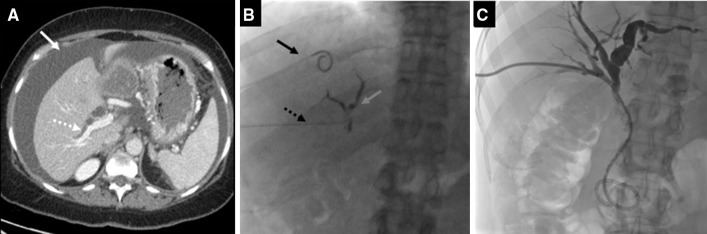
Methods: This is a multicenter prospective single-arm observational study conducted on patients affected by biliary tree stenosis/occlusion with jaundice and endoscopically inaccessible. The procedures have been performed puncturing the biliary system under US guidance and crossing the stenosis/occlusion under fluoroscopy. Beam-on time and X-ray dose have been evaluated.
Results: 117 patients affected by biliary tree stenosis/occlusion not manageable with an endoscopic approach have been included in this analysis. The biliary stenosis/occlusion was malignant in 90.8% and benign in 9.2%. Technical success, considered as positioning of a drainage tube into the biliary tree, was 100%. Overall clinical success, considered as decrease in total bilirubin level after a single procedure, was 95.7%. The overall mean number of liver punctures to catheterize the biliary tree was 1.57. The mean total beam-on time was 570.4 s; the mean dose-area product was 37.25 Gy cm2. No statistical significant differences were observed in terms of technical and dosimetry results according to right-sided and left-sided procedures. Complications rate recorded up to 30 days follow-up was 10.8%, all of minor grades.
Conclusions: In this series US guidance to access the biliary tree for PTBD was a safe and effective technique with an acceptable low-grade complications rate; the reported radiation dose is low.
Keywords: Biliary drainage; Complications; Percutaneous; Radiation dose; Ultrasound.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

Similar articles
-
Effectiveness of ultrasound-guided percutaneous transhepatic biliary drainage to reduce radiation exposure: A single-center experience.PLoS One. 2022 Nov 4;17(11):e0277272. doi: 10.1371/journal.pone.0277272. eCollection 2022. PLoS One. 2022. PMID: 36331963 Free PMC article.
-
Peripheral portal vein-oriented non-dilated bile duct puncture for percutaneous transhepatic biliary drainage.World J Gastroenterol. 2015 Nov 28;21(44):12628-34. doi: 10.3748/wjg.v21.i44.12628. World J Gastroenterol. 2015. PMID: 26640339 Free PMC article.
-
A comparative study of CT fluoroscopy combined with fluoroscopy versus fluoroscopy alone for percutaneous transhepatic biliary drainage.Cardiovasc Intervent Radiol. 2001 Jul-Aug;24(4):240-4. doi: 10.1007/s00270-001-0002-1. Cardiovasc Intervent Radiol. 2001. PMID: 11779013 Clinical Trial.
-
Endoscopic ultrasonography-guided biliary drainage: Who, when, which, and how?World J Gastroenterol. 2016 Jan 21;22(3):1297-303. doi: 10.3748/wjg.v22.i3.1297. World J Gastroenterol. 2016. PMID: 26811666 Free PMC article. Review.
-
Endoscopic Ultrasound-Guided Biliary Drainage.Gastrointest Endosc Clin N Am. 2018 Apr;28(2):171-185. doi: 10.1016/j.giec.2017.11.005. Epub 2018 Feb 3. Gastrointest Endosc Clin N Am. 2018. PMID: 29519330 Review.
Cited by
-
Is Ultrasound-guided Bedside Percutaneous Transhepatic Biliary Drainage Safe and Feasible in Critically Ill Patients with Severe Cholangitis? A Preliminary Single-center Experience.Indian J Crit Care Med. 2023 Jan;27(1):16-21. doi: 10.5005/jp-journals-10071-24379. Indian J Crit Care Med. 2023. PMID: 36756467 Free PMC article.
-
CIRSE Standards of Practice on Percutaneous Transhepatic Cholangiography, Biliary Drainage and Stenting.Cardiovasc Intervent Radiol. 2021 Oct;44(10):1499-1509. doi: 10.1007/s00270-021-02903-4. Epub 2021 Jul 29. Cardiovasc Intervent Radiol. 2021. PMID: 34327586
-
Effectiveness and complication rates of percutaneous transhepatic fluoroscopy-guided management of common bile duct stones: a single-arm meta-analysis.Eur Radiol. 2023 Nov;33(11):7398-7407. doi: 10.1007/s00330-023-09846-z. Epub 2023 Jun 16. Eur Radiol. 2023. PMID: 37326663
-
Ultrasound-guided Bedside Percutaneous Transhepatic Biliary Drainage in Critically Ill: A Friend Indeed.Indian J Crit Care Med. 2023 Jan;27(1):4-5. doi: 10.5005/jp-journals-10071-24393. Indian J Crit Care Med. 2023. PMID: 36756475 Free PMC article.
-
Analysis of the efficacy of Percutaneous Transhepatic Cholangiography Drainage (PTCD) and Endoscopic Retrograde Cholangiopancreatography (ERCP) in the treatment of Malignant Obstructive Jaundice (MOJ) in palliative drainage and preoperative biliary drainage: a single-center retrospective study.BMC Surg. 2024 Oct 12;24(1):307. doi: 10.1186/s12893-024-02595-w. BMC Surg. 2024. PMID: 39395969 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
