

Challenging the osseous component of sphenoorbital meningiomas
- PMID: 31368053
- PMCID: PMC6820812
- DOI: 10.1007/s00701-019-04015-y
Challenging the osseous component of sphenoorbital meningiomas
Abstract
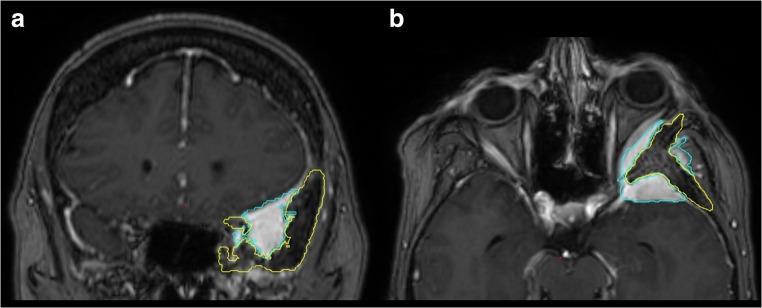
Background: Intraosseous growth is a unique feature of sphenoorbital meningiomas (SOM). Its close relation to neurovascular structures limits complete surgical resection and possibly contributes to the high recurrence rate.
Objective: To evaluate the growth behavior of intraosseous remnants and develop a protocol for precise intraoperative visualization of intraosseous SOM.
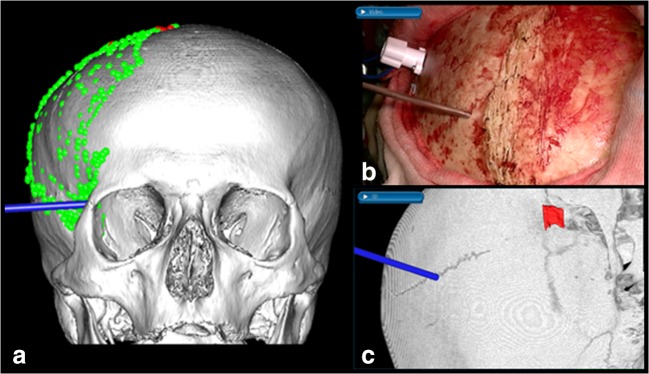
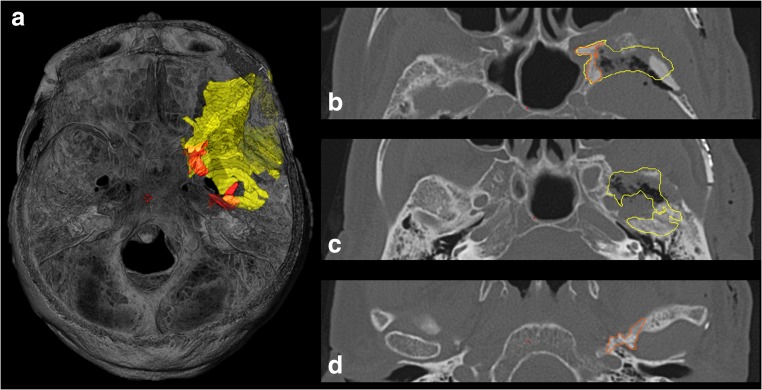
Methods: We included 31 patients operated for SOM from 2004 to 2017. The growth velocity of the intraosseous tumor component was volumetrically calculated in 20 cases. To improve accuracy of image guidance, we implemented a specialized bone surface-based registration algorithm. For intraoperative bone visualization, we included CT in multimodality continuous image guidance in 23 patients. The extent of resection (EOR) was compared with a standard MR-only navigation group (n = 8).
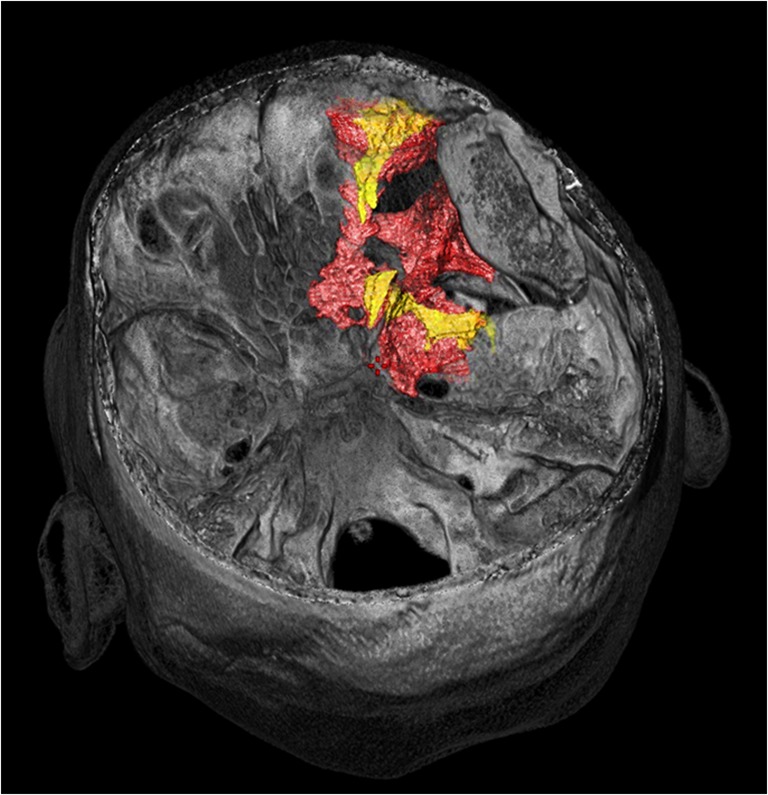
Results: In 11/20 cases (55%), a progressive regrowth of the intraosseous SOM remnant was noted during a mean follow-up of 52 months (range 20-132 months). We observed a mean increase of 6.2 cm3 (range 0.2-23.7 cm3) per patient and side during the follow-up period. Bone surface-based registration was significantly more accurate than skin surface-based registration (mean 0.7 ± 0.4 mm and 1.9 ± 0.7 mm, p < 0.001). The EOR of the intraosseous component was significantly higher using CT + MRI navigation compared with controls (96% vs. 81%, p = 0.044).
Conclusion: Quantitative assessment of the biological behavior of intraosseous remnants revealed a continuous slow growth rate independent of the soft tumor component of more than half of SOM. According to our data, application of a multimodal image guidance provided high accuracy and significantly increased the resection rate of the intraosseous component of SOM.
Keywords: Bone infiltration; Image guidance; Meningioma; Skull base; Sphenoorbital meningioma.
Conflict of interest statement
SW is an educational consultant and a technological advisory board member of Medtronic Navigation (Louisville, CO, USA). All other authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements) or nonfinancial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this manuscript.
Figures



References
-
- Cannon Paul S., Rutherford Scott A., Richardson Peter L., King Andrew, Leatherbarrow Brian. The Surgical Management and Outcomes for Spheno-orbital Meningiomas: A 7-year Review of Multi-disciplinary Practice. Orbit. 2009;28(6):371–376. - PubMed
-
- Pompili Alfredo, Derome Patrick J., Visot André, Guiot Gerard. Hyperostosing meningiomas of the sphenoid ridge—Clinical features, surgical therapy, and long-term observations: Review of 49 cases. Surgical Neurology. 1982;17(6):411–416. - PubMed
-
- Marcus Hani, Schwindack Christian, Santarius Thomas, Mannion Richard, Kirollos Ramez. Image-guided resection of spheno-orbital skull-base meningiomas with predominant intraosseous component. Acta Neurochirurgica. 2013;155(6):981–988. - PubMed
-
- Freeman Jacob L., Davern Monica S., Oushy Soliman, Sillau Stefan, Ormond D. Ryan, Youssef A. Samy, Lillehei Kevin O. Spheno-Orbital Meningiomas: A 16-Year Surgical Experience. World Neurosurgery. 2017;99:369–380. - PubMed
-
- Shrivastava Raj K., Sen Chandranath, Costantino Peter D., Della Rocca Robert. Sphenoorbital meningiomas: surgical limitations and lessons learned in their long-term management. Journal of Neurosurgery. 2005;103(3):491–497. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
