

The efficacy of HBOC-201 in ex situ gradual rewarming kidney perfusion in a rat model
- PMID: 31368159
- PMCID: PMC6916591
- DOI: 10.1111/aor.13534
The efficacy of HBOC-201 in ex situ gradual rewarming kidney perfusion in a rat model
Abstract
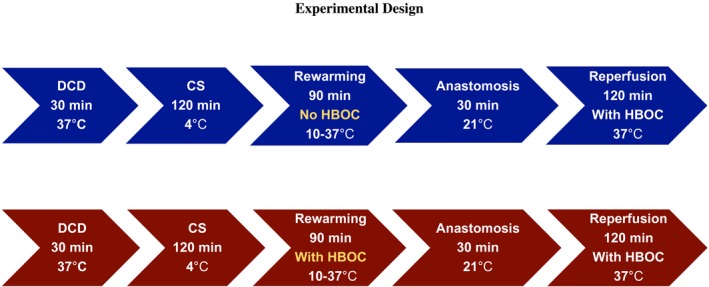
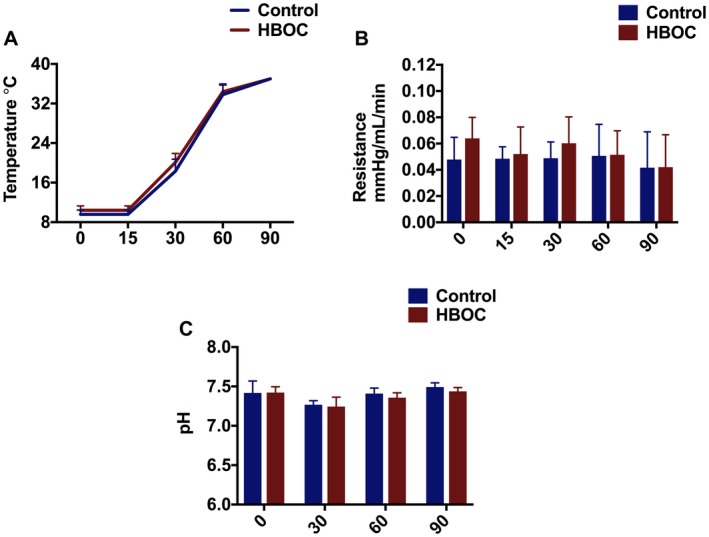
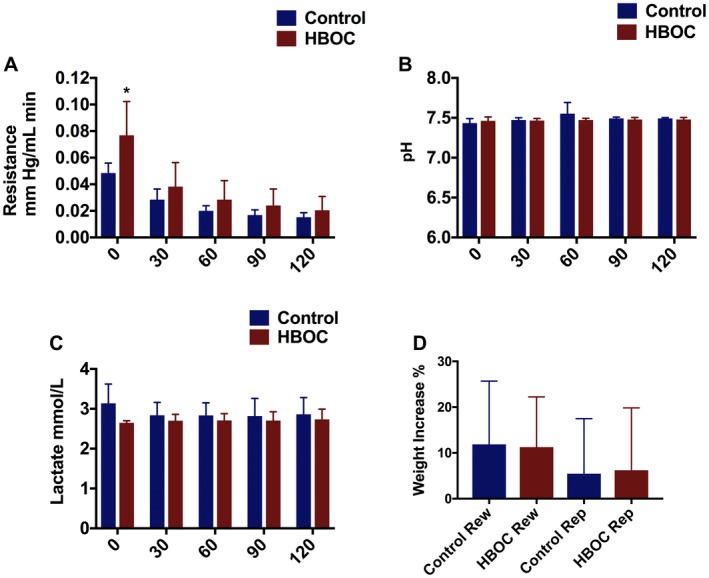
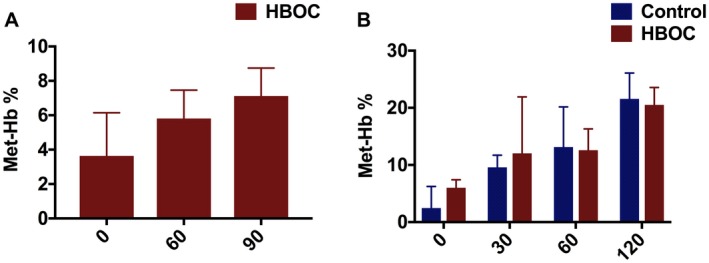
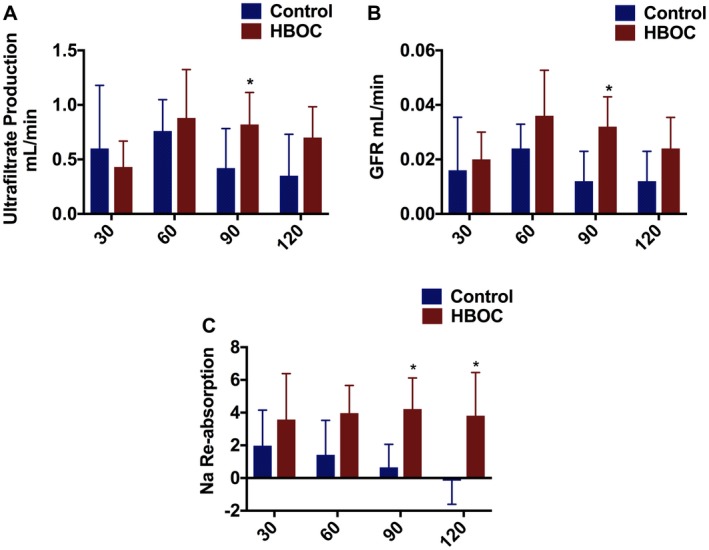
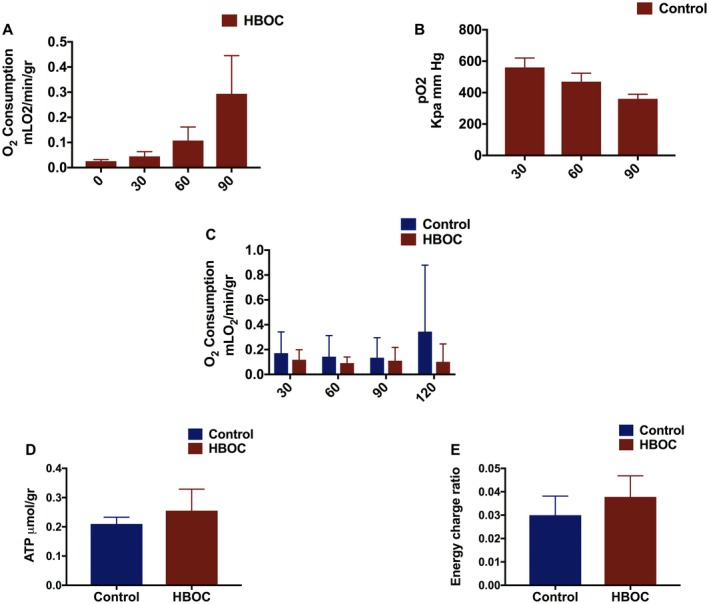
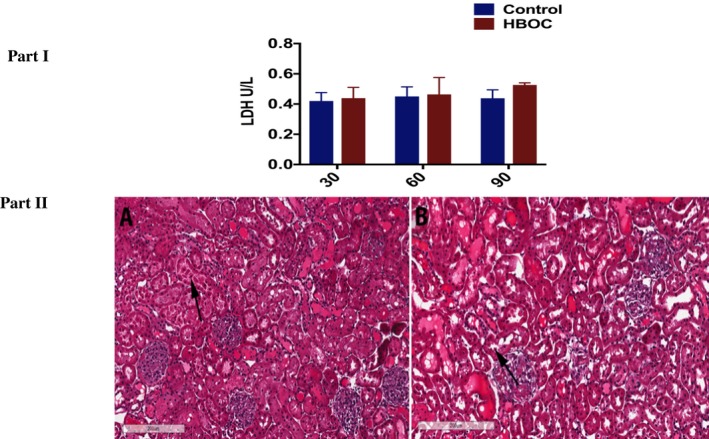
Gradual rewarming from hypothermic to normothermic is a novel perfusion modality with superior outcome to sudden rewarming to normothermic. However, the identification of an oxygen carrier that could function at a temperature range from 4 to 7°C or whether it is necessary to use oxygen carrier during kidney rewarming, remains unresolved. This study was designed to test the use of a hemoglobin-based oxygen carrier (HBOC) during gradual kidney rewarming as an alternative to simple dissolved oxygen. In this study, 10 rat kidneys were randomly divided into the control and the HBOC group. In the control group, no oxygen carrier was used during rewarming perfusion and the perfusion solution was oxygenated only by applying diffused carbogen flow. The protocol mimicked a donor after circulatory death (DCD) kidney transplantation, where after 30 minutes warm ischemia and 120 minutes cold storage in University of Wisconsin solution, the DCD kidneys underwent gradual rewarming from 10 to 37°C during 90 minutes with or without HBOC. This was followed by 30 minutes of warm ischemia in room temperature to mimic the anastomosis time and 120 minutes of reperfusion at 37°C to mimic the early post-transplant state of the graft. The HBOC group demonstrated superior kidney function which was highlighted by higher ultrafiltrate production, better glomerular filtration rate and improved sodium reabsorption. There was no significant difference between the 2 groups regarding the hemodynamics, tissue injury, and adenosine triphosphate levels. In conclusion, this study suggests better renal function recovery in DCD kidneys after rewarming with HBOC compared to rewarming without an oxygen carrier.
Keywords: donor after circulatory death kidney graft; hemoglobin-based oxygen carrier; oxygen carrier; perfusion; rewarming perfusion.
© 2019 The Authors. Artificial Organs published by Wiley Periodicals, Inc., on behalf of International Center for Artificial Organ and Transplantation (ICAOT).
Conflict of interest statement
The authors of this manuscript have conflicts of interest to disclose: Dr. Uygun is inventor on pending patents relevant to this study. Dr. Uygun has a financial interest in Organ Solutions, a company focused on developing organ preservation technology. Dr. Uygun's interests are managed by the MGH and Partners HealthCare in accordance with their conflict of interest policies. Drs. Tessier and Uygun have several IP disclosures on extended organ preservation that may be relevant to this study. The HOBC‐201 used in this study was provided by HBO2 Therapeutics LLC.
Figures
References
-
- Op den Dries S, Karimian N, Porte RJ. Normothermic machine perfusion of discarded liver grafts. Am J Transplant Off J Am Soc Transplant Am Soc Transpl Surg. 2013;13:2504. - PubMed
-
- Westerkamp AC, Mahboub P, Meyer SL, Hottenrott M, Ottens PJ, Wiersema‐Buist J, et al. End‐ischemic machine perfusion reduces bile duct injury in donation after circulatory death rat donor livers independent of the machine perfusion temperature. Liver Transplant Off Publ Am Assoc Study Liver Dis Int Liver Transplant Soc. 2015;21:1300–11. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
