

Evaluation and Management of Obesity Hypoventilation Syndrome. An Official American Thoracic Society Clinical Practice Guideline
- PMID: 31368798
- PMCID: PMC6680300
- DOI: 10.1164/rccm.201905-1071ST
Evaluation and Management of Obesity Hypoventilation Syndrome. An Official American Thoracic Society Clinical Practice Guideline
Erratum in
-
Erratum: Evaluation and Management of Obesity Hypoventilation Syndrome. An Official American Thoracic Society Clinical Practice Guideline.Am J Respir Crit Care Med. 2019 Nov 15;200(10):1326. doi: 10.1164/rccm.v200erratum7. Am J Respir Crit Care Med. 2019. PMID: 31729906 Free PMC article. No abstract available.
Abstract
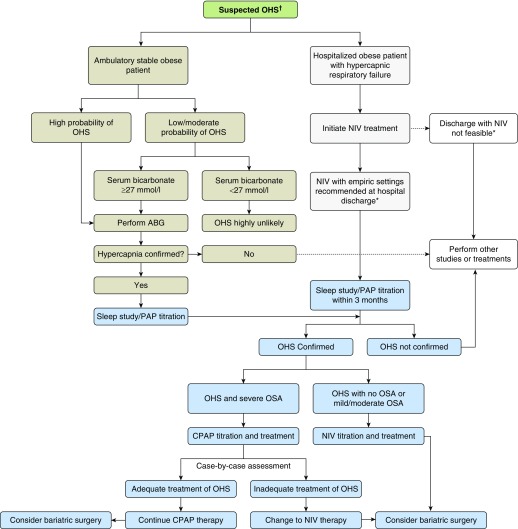
Background: The purpose of this guideline is to optimize evaluation and management of patients with obesity hypoventilation syndrome (OHS).Methods: A multidisciplinary panel identified and prioritized five clinical questions. The panel performed systematic reviews of available studies (up to July 2018) and followed the Grading of Recommendations, Assessment, Development, and Evaluation evidence-to-decision framework to develop recommendations. All panel members discussed and approved the recommendations.Recommendations: After considering the overall very low quality of the evidence, the panel made five conditional recommendations. We suggest that: 1) clinicians use a serum bicarbonate level <27 mmol/L to exclude the diagnosis of OHS in obese patients with sleep-disordered breathing when suspicion for OHS is not very high (<20%) but to measure arterial blood gases in patients strongly suspected of having OHS, 2) stable ambulatory patients with OHS receive positive airway pressure (PAP), 3) continuous positive airway pressure (CPAP) rather than noninvasive ventilation be offered as the first-line treatment to stable ambulatory patients with OHS and coexistent severe obstructive sleep apnea, 4) patients hospitalized with respiratory failure and suspected of having OHS be discharged with noninvasive ventilation until they undergo outpatient diagnostic procedures and PAP titration in the sleep laboratory (ideally within 2-3 mo), and 5) patients with OHS use weight-loss interventions that produce sustained weight loss of 25% to 30% of body weight to achieve resolution of OHS (which is more likely to be obtained with bariatric surgery).Conclusions: Clinicians may use these recommendations, on the basis of the best available evidence, to guide management and improve outcomes among patients with OHS.
Keywords: Pickwickian; bilevel PAP; chronic hypercapnic respiratory failure; hypercapnia; sleep-disordered breathing.
Figures
Comment in
-
Clinical Practice Guideline Summary for Clinicians: Evaluation and Management of Obesity Hypoventilation Syndrome.Ann Am Thorac Soc. 2020 Jan;17(1):11-15. doi: 10.1513/AnnalsATS.201908-579CME. Ann Am Thorac Soc. 2020. PMID: 31661315 No abstract available.
References
-
- Randerath W, Verbraecken J, Andreas S, Arzt M, Bloch KE, Brack T, et al. Definition, discrimination, diagnosis and treatment of central breathing disturbances during sleep. Eur Respir J. 2017;49:1600959. - PubMed
-
- Masa JF, Corral J, Romero A, Caballero C, Terán-Santos J, Alonso-Álvarez ML, et al. Spanish Sleep Network(*) Protective cardiovascular effect of sleep apnea severity in obesity hypoventilation syndrome. Chest. 2016;150:68–79. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
