

Progression of Stargardt Disease as Determined by Fundus Autofluorescence Over a 12-Month Period: ProgStar Report No. 11
- PMID: 31369039
- PMCID: PMC6681653
- DOI: 10.1001/jamaophthalmol.2019.2885
Progression of Stargardt Disease as Determined by Fundus Autofluorescence Over a 12-Month Period: ProgStar Report No. 11
Abstract
Importance: Sensitive outcome measures for disease progression are needed for treatment trials of Stargardt disease.
Objective: To estimate the progression rate of atrophic lesions in the prospective Natural History of the Progression of Atrophy Secondary to Stargardt Disease (ProgStar) study over a 12-month period.
Design, setting, and participants: This multicenter prospective cohort study was conducted in an international selection of tertiary referral centers from October 21, 2013, to February 15, 2017. Patients who were affected by Stargardt disease, aged 6 years and older at baseline, and harboring disease-causing variants of the ABCA4 gene were enrolled at 9 centers in the United States, United Kingdom, and continental Europe. Data analysis occurred from November 2016 to January 2017.
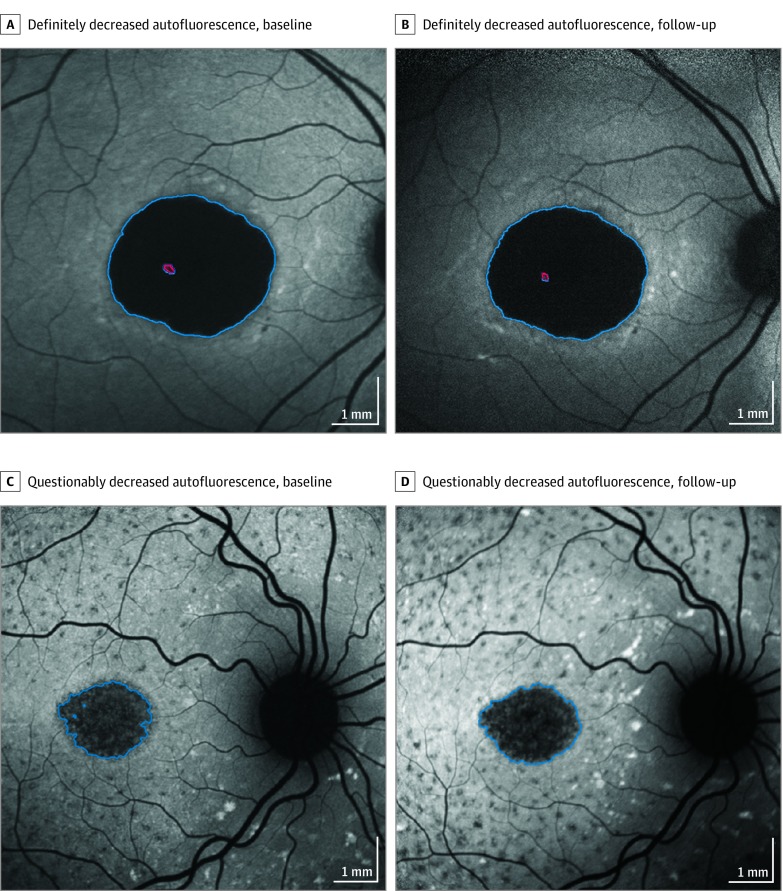
Exposures: Autofluorescence images obtained with a standard protocol were sent to a central reading center, and areas of definitely decreased autofluorescence, questionably decreased autofluorescence, and the total combined area of decreased autofluorescence were outlined and quantified. Progression rates were estimated from linear mixed models with time as the independent variable.
Main outcomes and measures: Yearly rate of progression, using the growth of atrophic lesions measured by autofluorescence imaging.
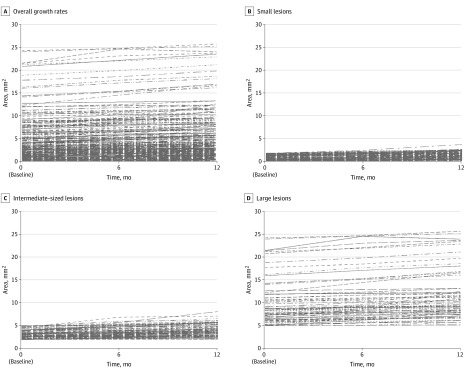
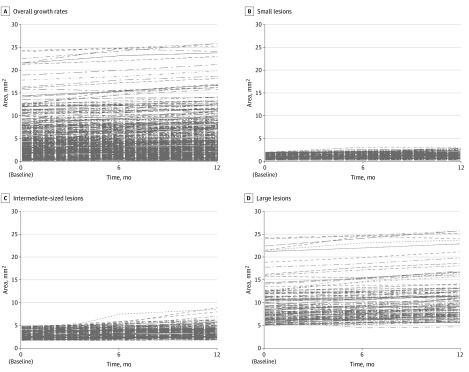
Results: A total of 259 study participants (488 eyes; 230 individuals [88.8%] were examined in both eyes) were enrolled (mean [SD] age at first visit, 33.3 [15.1] years; 118 [54.4%] female). Gradable images were available for evaluation for 480 eyes at baseline and 454 eyes after 12 months. At baseline, definitely decreased autofluorescence was present in 306 eyes, and the mean (SD) lesion size was 3.93 (4.37) mm2. The mean total area of decreased autofluorescence at baseline was 4.07 (4.04) mm2. The estimated progression of definitely decreased autofluorescence was 0.76 (95% CI, 0.54-0.97) mm2 per year (P < .001), and the total area of both questionably and definitely decreased autofluorescence was 0.64 (95% CI, 0.50-0.78) mm2 per year (P < .001). Both progression rates depended on initial lesion size.
Conclusions and relevance: In Stargardt disease, autofluorescence imaging may serve as a monitoring tool and definitely decreased autofluorescence and total area as outcome measures for interventional clinical trials that aim to slow disease progression. Rates of progression depended mainly on initial lesion size.
Conflict of interest statement
Figures
Comment in
References
-
- Strauss RW, Ho A, Muñoz B, et al. ; Progression of Stargardt Disease Study Group . The natural history of the progression of atrophy secondary to Stargardt disease (ProgStar) studies: design and baseline characteristics, ProgStar report No. 1. Ophthalmology. 2016;123(4):817-828. doi:10.1016/j.ophtha.2015.12.009 - DOI - PubMed
