

Evidence-based recommendations for energy intake in pregnant women with obesity
- PMID: 31369400
- PMCID: PMC6819141
- DOI: 10.1172/JCI130341
Evidence-based recommendations for energy intake in pregnant women with obesity
Abstract
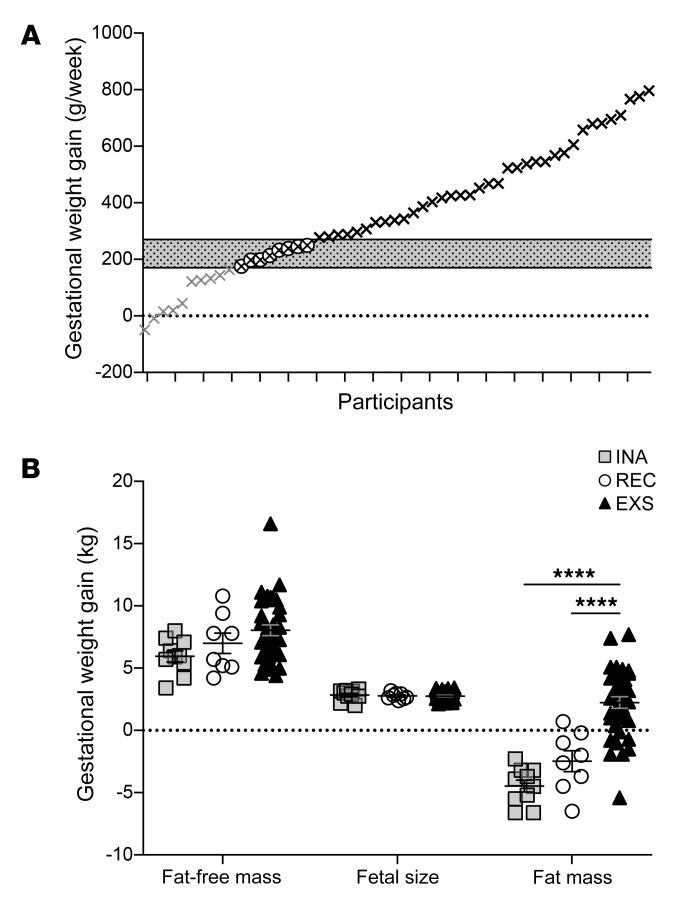
Background: In women with obesity, excess gestational weight gain (≥270 g/week) occurs in two out of three pregnancies and contributes to metabolic impairments in both mother and baby. To improve obstetrical care, objectively assessed information on energy balance is urgently needed. The objective of this study was to characterize determinants of gestational weight gain in women with obesity.
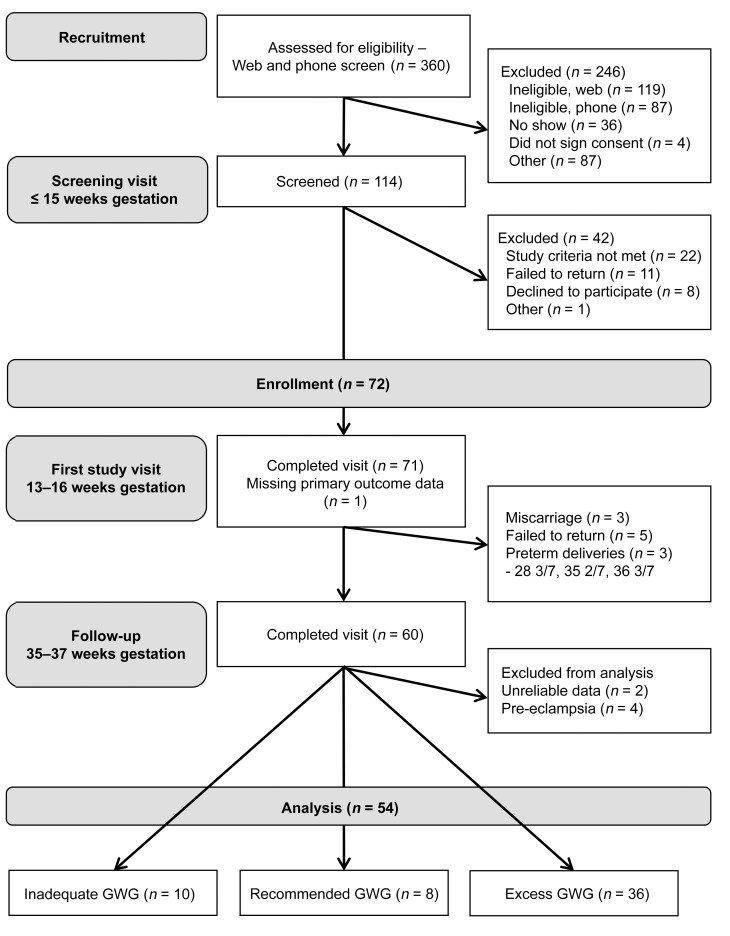
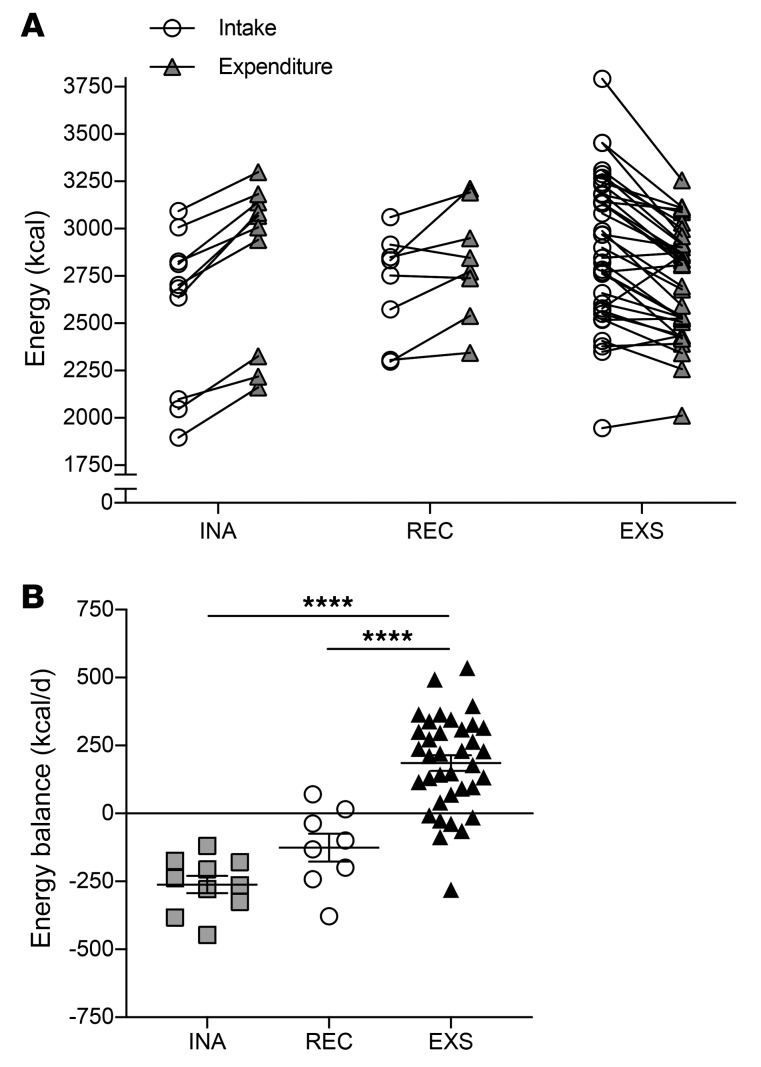
Methods: This was a prospective, observational study of pregnant women with obesity. The primary outcome was energy intake calculated by the energy intake-balance method. Energy expenditure was measured by doubly-labeled water and whole-room indirect calorimetry and body composition as 3-compartment model by air displacement plethysmography and isotope dilution in early (13-16 weeks) and late pregnancy (35-37 weeks).
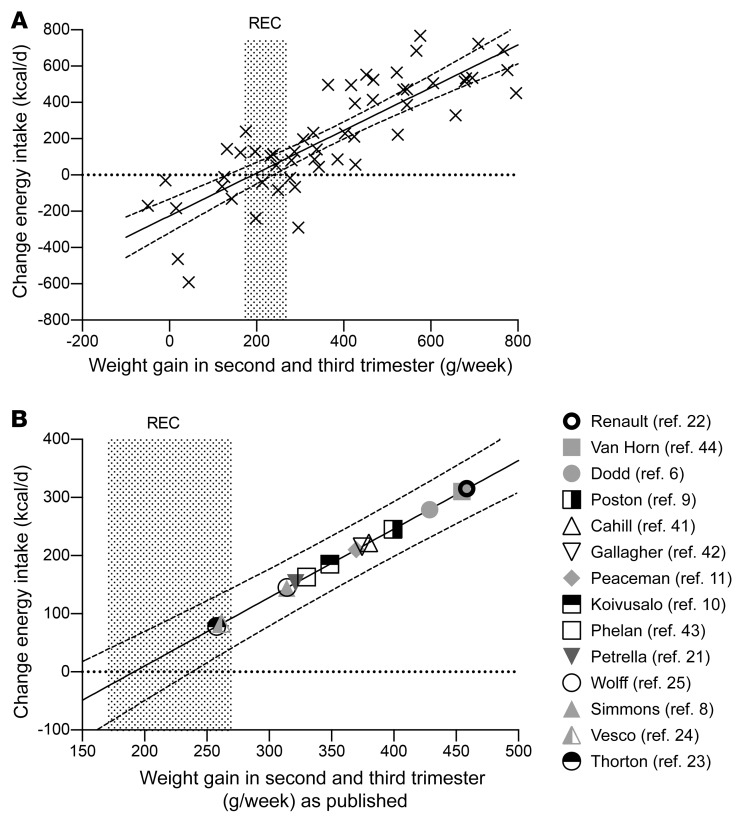
Results: In pregnant women with obesity (n=54), recommended weight gain (n=8, 15%) during the second and third trimesters was achieved when energy intake was 125±52 kcal/d less than energy expenditure. In contrast, women with excess weight gain (67%) consumed 186±29 kcal/d more than they expended (P<0.001). Energy balance affected maternal adiposity (recommended: -2.5±0.8 kg fat mass, excess: +2.2±0.5, inadequate: -4.5±0.5, P<0.001), but not fetal growth. Weight gain was not related to demographics, activity, metabolic biomarkers, or diet quality. We estimated that energy intake requirements for recommended weight gain during the second and third trimesters were not increased as compared to energy requirements early in pregnancy (34±53 kcal/d, P=0.83).
Conclusions: We here provide the first evidence-based recommendations for energy intake in pregnant women with obesity. Contrary to current recommendations, energy intake should not exceed energy expenditure.
Funding: This study was funded by the National Institutes of Health (R01DK099175; Redman, U54GM104940 and P30DK072476; Core support).
Trial registration: clinicaltrials.gov: NCT01954342.
Keywords: Clinical practice; Metabolism; Obesity; Obstetrics/gynecology; Reproductive Biology.
Conflict of interest statement
Figures
Comment in
-
Time to change weight gain recommendations for pregnant women with obesity.J Clin Invest. 2019 Nov 1;129(11):4567-4569. doi: 10.1172/JCI131932. J Clin Invest. 2019. PMID: 31545296 Free PMC article.
References
-
- Institute of Medicine (US) National Research Council (US) Committee to Reexamine IOM Pregnancy Weight Guidelines. In: Rasmussen KM, Yaktine AL, eds. Weight Gain During Pregnancy: Reexamining the Guidelines. Washington (DC); 2009.
-
- Mamun AA, Kinarivala M, O’Callaghan MJ, Williams GM, Najman JM, Callaway LK. Associations of excess weight gain during pregnancy with long-term maternal overweight and obesity: evidence from 21 y postpartum follow-up. Am J Clin Nutr. 2010;91(5):1336–1341. doi: 10.3945/ajcn.2009.28950. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
