

Ventilation Rates and Pediatric In-Hospital Cardiac Arrest Survival Outcomes
- PMID: 31369424
- PMCID: PMC7898415
- DOI: 10.1097/CCM.0000000000003898
Ventilation Rates and Pediatric In-Hospital Cardiac Arrest Survival Outcomes
Abstract
Objectives: The objective of this study was to associate ventilation rates during in-hospital cardiopulmonary resuscitation with 1) arterial blood pressure during cardiopulmonary resuscitation and 2) survival outcomes.
Design: Prospective, multicenter observational study.
Setting: Pediatric and pediatric cardiac ICUs of the Collaborative Pediatric Critical Care Research Network.
Patients: Intubated children (≥ 37 wk gestation and < 19 yr old) who received at least 1 minute of cardiopulmonary resuscitation.
Interventions: None.
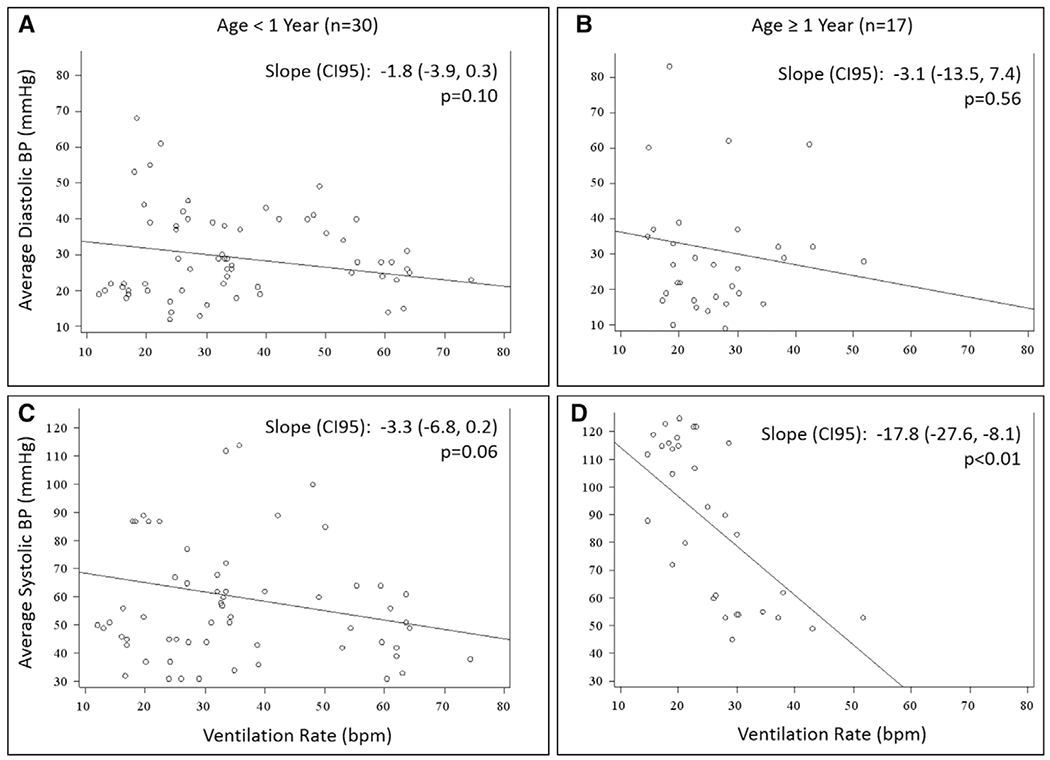
Measurements and main results: Arterial blood pressure and ventilation rate (breaths/min) were manually extracted from arterial line and capnogram waveforms. Guideline rate was defined as 10 ± 2 breaths/min; high ventilation rate as greater than or equal to 30 breaths/min in children less than 1 year old, and greater than or equal to 25 breaths/min in older children. The primary outcome was survival to hospital discharge. Regression models using Firth penalized likelihood assessed the association between ventilation rates and outcomes. Ventilation rates were available for 52 events (47 patients). More than half of patients (30/47; 64%) were less than 1 year old. Eighteen patients (38%) survived to discharge. Median event-level average ventilation rate was 29.8 breaths/min (interquartile range, 23.8-35.7). No event-level average ventilation rate was within guidelines; 30 events (58%) had high ventilation rates. The only significant association between ventilation rate and arterial blood pressure occurred in children 1 year old or older and was present for systolic blood pressure only (-17.8 mm Hg/10 breaths/min; 95% CI, -27.6 to -8.1; p < 0.01). High ventilation rates were associated with a higher odds of survival to discharge (odds ratio, 4.73; p = 0.029). This association was stable after individually controlling for location (adjusted odds ratio, 5.97; p = 0.022), initial rhythm (adjusted odds ratio, 3.87; p = 0.066), and time of day (adjusted odds ratio, 4.12; p = 0.049).
Conclusions: In this multicenter cohort, ventilation rates exceeding guidelines were common. Among the range of rates delivered, higher rates were associated with improved survival to hospital discharge.
Figures

Comment in
-
The Perceived Impact of Ventilation Rate on Cardiac Arrest Outcomes: Does It Matter?Crit Care Med. 2019 Nov;47(11):1672-1673. doi: 10.1097/CCM.0000000000003982. Crit Care Med. 2019. PMID: 31609270 No abstract available.
-
High Ventilation Rates May Be Not Optimal.Crit Care Med. 2020 Feb;48(2):e160. doi: 10.1097/CCM.0000000000004066. Crit Care Med. 2020. PMID: 31939824 No abstract available.
-
The authors reply.Crit Care Med. 2020 Feb;48(2):e160-e161. doi: 10.1097/CCM.0000000000004100. Crit Care Med. 2020. PMID: 31939825 No abstract available.
References
-
- Knudson JD, Neish SR, Cabrera AG, et al.: Prevalence and outcomes of pediatric in-hospital cardiopulmonary resuscitation in the United States: An analysis of the Kids’ Inpatient Database. Crit Care Med 2012; 40:2940–2944 - PubMed
-
- Nadkarni VM, Larkin GL, Peberdy MA, et al.; National Registry of Cardiopulmonary Resuscitation Investigators: First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults. JAMA 2006; 295:50–57 - PubMed
Publication types
MeSH terms
Grants and funding
- U10 HD050012/HD/NICHD NIH HHS/United States
- UG1 HD050012/HD/NICHD NIH HHS/United States
- UG1 HD049983/HD/NICHD NIH HHS/United States
- UG1 HD050096/HD/NICHD NIH HHS/United States
- P2C HD047879/HD/NICHD NIH HHS/United States
- U10 HD063106/HD/NICHD NIH HHS/United States
- UG1 HD063108/HD/NICHD NIH HHS/United States
- RL1 HD107773/HD/NICHD NIH HHS/United States
- UG1 HD063106/HD/NICHD NIH HHS/United States
- UG1 HD083171/HD/NICHD NIH HHS/United States
- U10 HD063114/HD/NICHD NIH HHS/United States
- U01 HD049934/HD/NICHD NIH HHS/United States
- UG1 HD049981/HD/NICHD NIH HHS/United States
- UG1 HD083170/HD/NICHD NIH HHS/United States
- UG1 HD083166/HD/NICHD NIH HHS/United States
