

Determining the Generalizability of the PROMIS Depression Domain's Floor Effect and Completion Time in Patients Undergoing Orthopaedic Surgery
- PMID: 31369439
- PMCID: PMC6999924
- DOI: 10.1097/CORR.0000000000000782
Determining the Generalizability of the PROMIS Depression Domain's Floor Effect and Completion Time in Patients Undergoing Orthopaedic Surgery
Abstract
Background: Depression is common and can decrease the likelihood that a patient undergoing an orthopaedic procedure will improve after that intervention. Research at a single institution using the Patient-reported Outcomes Measurement Information System (PROMIS) showed that the PROMIS Depression domain had a substantial floor effect (lowest depressive symptoms measurable) in patients with orthopaedic conditions, although the instrument is designed to follow a population-based normal distribution. Patients with the lowest scores (floor) completed the questionnaire more quickly than those who did not have the lowest scores, which suggests that patients may not want to report or discuss depressive symptoms with their orthopaedic surgeon.
Questions/purposes: (1) Do the scores of a large population of patients with orthopaedic conditions completing the PROMIS Physical Function (PF), Pain Interference (PI), and Depression questionnaires follow the normal population distribution used to calibrate the PROMIS instrument? (2) Do the scores of a large population of patients with foot and ankle, spine, upper extremity, multiple orthopaedic subspecialty, or other orthopaedic conditions completing the PROMIS Depression questionnaire follow the normal population distribution used to calibrate the PROMIS instrument? (3) Do all orthopaedic patients with the lowest possible score (floor effect) on the PROMIS Depression questionnaire answer questions more quickly than those who do not?
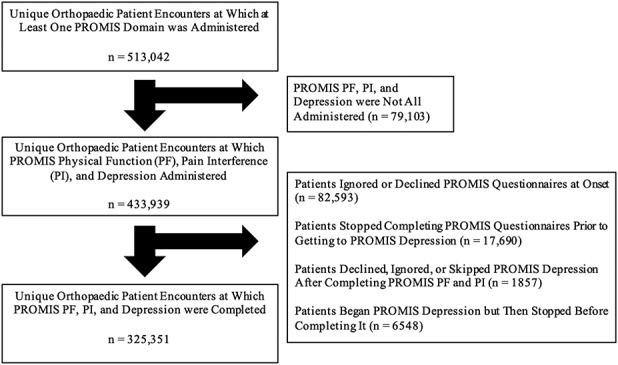
Methods: Between February 12, 2015 and July 19, 2018, a total of 513,042 patients with orthopaedic conditions at a single urban, tertiary academic medical center were asked to complete the PROMIS PF, PI, and Depression domains. The PROMIS PF, PI, and Depression questionnaires were administered at 433,939 patient encounters (85%), and 325,251 of 433,939 (75%) completed all three questionnaires and were included in our final sample. The remaining encounters were excluded from all analyses because of incomplete PROMIS data. Using this large sample size, we determined the distributions of the PROMIS PF, PI, and Depression domains for all patients with orthopaedic conditions by visual inspection. We calculated the percentage of patients with the lowest possible score on the PROMIS Depression domain ("floor group") for all patients with orthopaedic conditions, as well for patients presenting to orthopaedic subspecialists (foot and ankle, spine, upper extremity, multiple subspecialties, or other specialists). We compared patient and PROMIS characteristics between patients in the floor group and all others ("standard group") using a bivariate analysis, including the total time it took to complete the questionnaires and average time it took to answer each question.
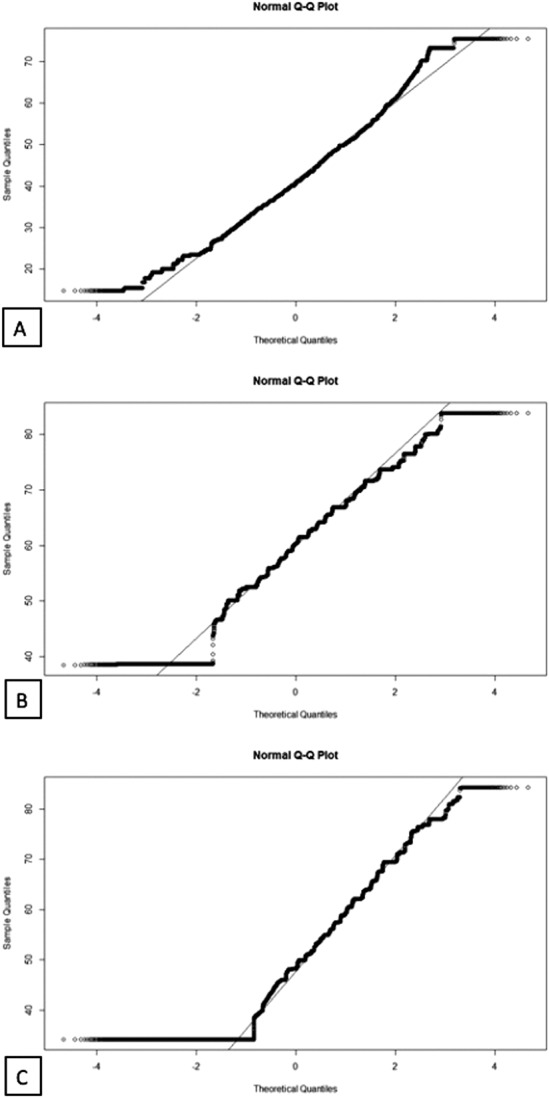
Results: Of the three PROMIS domains analyzed, only the PROMIS PF demonstrated a normal distribution on visual inspection. PROMIS PI scores had a measurable ceiling effect (more pain symptoms) (15,520 of 325,251 patient encounters; 5%), while PROMIS Depression scores demonstrated a clear floor effect (65,226 of 325,251; 20%). When analyzed by subspecialty, there was a clear floor effect for the PROMIS Depression in the specialties of foot and ankle (6031 of 29,273 patient encounters; 21%), spine (7611 of 58,266; 13%), upper extremity (9851 of 42,864; 23%), multiple subspecialties (276 of 1662; 17%), and other (41, 454 of 193,185; 22%). Generally, those in the floor group spent less time per question on the PROMIS Depression questionnaire than did those in the standard group (5.3 seconds ± 2.6 seconds versus 8.1 seconds ± 4.6 seconds; mean difference, 2.8 seconds; p < 0.001).
Conclusions: The substantial floor effect of the PROMIS Depression in the setting of hasty completion raises the question of whether such results truly indicate that these patients have minimal depression or whether they simply do not report their true mental health status in an orthopaedic setting. When such patients are seen in clinic, surgeons may benefit from using the PROMIS Depression as an educational opportunity to explain the importance of mental health in orthopaedic care and ensure the questionnaire is completed accurately. This study builds on previous work by suggesting these findings apply to other general and subspecialty orthopaedic patient populations at academic medical centers. Future work may seek to determine the best way of ensuring that the PROMIS Depression questionnaire is completed accurately in orthopaedic clinics.
Level of evidence: Level II, diagnostic study.
Conflict of interest statement
All ICMJE Conflict of Interest Forms for authors and
Figures
Comment in
-
CORR Insights®: Determining the Generalizability of the PROMIS Depression Domain's Floor Effect and Completion Time in Patients Undergoing Orthopaedic Surgery.Clin Orthop Relat Res. 2019 Oct;477(10):2226-2227. doi: 10.1097/CORR.0000000000000829. Clin Orthop Relat Res. 2019. PMID: 31169626 Free PMC article. No abstract available.
Similar articles
-
Do Patient Sociodemographic Factors Impact the PROMIS Scores Meeting the Patient-Acceptable Symptom State at the Initial Point of Care in Orthopaedic Foot and Ankle Patients?Clin Orthop Relat Res. 2019 Nov;477(11):2555-2565. doi: 10.1097/CORR.0000000000000866. Clin Orthop Relat Res. 2019. PMID: 31261259 Free PMC article.
-
Floor Effect of PROMIS Depression CAT Associated With Hasty Completion in Orthopaedic Surgery Patients.Clin Orthop Relat Res. 2018 Apr;476(4):696-703. doi: 10.1007/s11999.0000000000000076. Clin Orthop Relat Res. 2018. PMID: 29419628 Free PMC article.
-
What is the Impact of Social Deprivation on Physical and Mental Health in Orthopaedic Patients?Clin Orthop Relat Res. 2019 Aug;477(8):1825-1835. doi: 10.1097/CORR.0000000000000698. Clin Orthop Relat Res. 2019. PMID: 31107333 Free PMC article.
-
What Are the Floor and Ceiling Effects of Patient-Reported Outcomes Measurement Information System Computer Adaptive Test Domains in Orthopaedic Patients? A Systematic Review.Arthroscopy. 2020 Mar;36(3):901-912.e7. doi: 10.1016/j.arthro.2019.09.022. Epub 2020 Jan 7. Arthroscopy. 2020. PMID: 31919023
-
The promise of computer adaptive testing in collection of orthopaedic outcomes: an evaluation of PROMIS utilization.J Patient Rep Outcomes. 2022 Jan 4;6(1):2. doi: 10.1186/s41687-021-00407-w. J Patient Rep Outcomes. 2022. PMID: 34982280 Free PMC article. Review.
Cited by
-
CORR Insights®: Determining the Generalizability of the PROMIS Depression Domain's Floor Effect and Completion Time in Patients Undergoing Orthopaedic Surgery.Clin Orthop Relat Res. 2019 Oct;477(10):2226-2227. doi: 10.1097/CORR.0000000000000829. Clin Orthop Relat Res. 2019. PMID: 31169626 Free PMC article. No abstract available.
-
What factors are associated with perceived disease onset in patients with hip and knee osteoarthritis?J Orthop. 2021 Jul 14;26:88-93. doi: 10.1016/j.jor.2021.07.013. eCollection 2021 Jul-Aug. J Orthop. 2021. PMID: 34341628 Free PMC article.
-
Delivery of Hand Care to Patients With High Anxiety Burden.J Hand Surg Am. 2024 Dec;49(12):1212-1218. doi: 10.1016/j.jhsa.2024.08.005. Epub 2024 Sep 21. J Hand Surg Am. 2024. PMID: 39306772 Free PMC article.
-
Mental Health Among People Presenting for Care of Physical Symptoms: The Factors Associated with Suicidality and Symptoms of Depression and Anxiety are Similar Across Specialties.Chronic Stress (Thousand Oaks). 2023 Apr 18;7:24705470231169106. doi: 10.1177/24705470231169106. eCollection 2023 Jan-Dec. Chronic Stress (Thousand Oaks). 2023. PMID: 37101814 Free PMC article.
-
PROMIS Global Physical Health Subscale Strongly Correlates and Performs Similarly to the QuickDASH in Hand and Upper Extremity Patients.Hand (N Y). 2025 May;20(3):487-491. doi: 10.1177/15589447231211603. Epub 2023 Nov 14. Hand (N Y). 2025. PMID: 37961854 Free PMC article.
References
-
- Adogwa O, Parker SL, Shau DN, Mendenhall SK, Bydon A, Cheng JS, Asher AL, McGirt MJ. Preoperative Zung depression scale predicts patient satisfaction independent of the extent of improvement after revision lumbar surgery. Spine J. 2013;13:501-506. - PubMed
-
- Ardern CL, Taylor NF, Feller JA, Whitehead TS, Webster KE. Psychological responses matter in returning to preinjury level of sport after anterior cruciate ligament reconstruction surgery. Am J Sports Med. 2013;41:1549-1558. - PubMed
-
- Bernstein DN, Kelly M, Houck JR, Ketz JP, Flemister AS, DiGiovanni BF, Baumhauer JF, Oh I. PROMIS Pain Interference is superior vs numeric pain rating scale for pain assessment in foot and ankle patients. Foot Ankle Int. 2019;40:139-144. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
