

Increasing metabolic co-morbidities are associated with higher risk of advanced fibrosis in nonalcoholic steatohepatitis
- PMID: 31369606
- PMCID: PMC6675045
- DOI: 10.1371/journal.pone.0220612
Increasing metabolic co-morbidities are associated with higher risk of advanced fibrosis in nonalcoholic steatohepatitis
Abstract
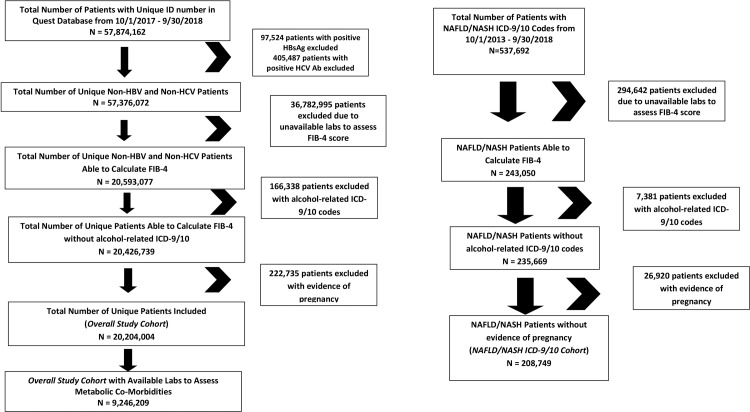
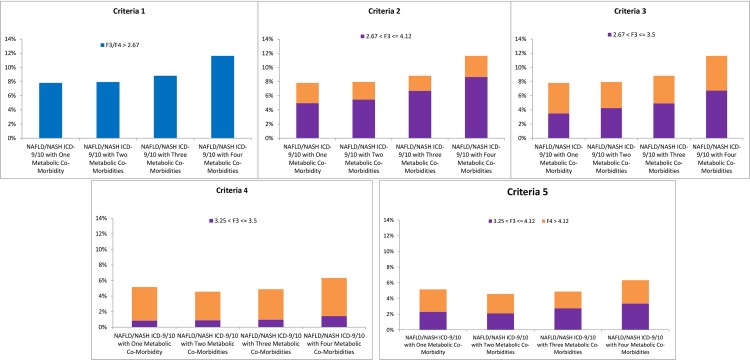
Hepatic fibrosis and advanced fibrosis in particular is the strongest predictor of liver-related outcomes and mortality among nonalcoholic steatohepatitis (NASH) patients. Understanding prevalence and predictors of NASH with advanced fibrosis is critical for healthcare resource planning. Using a large U.S. clinical laboratory database from 10/1/2017-9/30/2018, adults negative for hepatitis B and hepatitis C and after excluding for alcoholic liver disease and pregnancy were evaluated for prevalence of F3 and F4 fibrosis using a systematic algorithm of five fibrosis-4 (FIB-4) criteria: Criteria 1 (≥F3: >2.67), Criteria 2 (2.67<F3≤4.12 and F4>4.12), Criteria 3 (2.67<F3≤3.15, F4>3.15), Criteria 4 (3.25<F3≤3.5, F4>3.5), Criteria 5 (3.25<F3≤4.12, F4>4.12). Metabolic co-morbidities evaluated included decreased high density lipoprotein (<40 mg/dL men, <50 mg/dL women), high triglycerides (≥150 mg/dL), elevated hemoglobin A1C (≥6.5%). Parallel analyses of patients with specific NAFLD/NASH ICD-9/10 codes from 10/1/2013-9/30/2018 were performed. Multivariate logistic regression models evaluated for predictors of ≥F3 fibrosis. Among patients with NAFLD/NASH ICD-9/10 codes, ≥F3 prevalence ranged from 4.35% - 6.90%, and F4 prevalence ranged from 2.52%- 3.67%. Increasing metabolic co-morbidities was associated with higher risk of ≥F3 fibrosis. Compared to NASH patients without metabolic co-morbidities, NASH with four concurrent metabolic co-morbidities had higher risk of ≥F3 (OR 1.56, 95% CI 1.40-1.73, p<0.001). In summary, prevalence of NASH with advanced fibrosis among U.S. adults was as high as 6.90% and prevalence of NASH with cirrhosis was as high as 3.67%, representing 5.18 million and 2.75 million, respectively, when using an estimate of 75 million U.S. adults with NAFLD. Co-morbid metabolic abnormalities were associated with higher risk of advanced fibrosis among NASH patients.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: Robert Wong: research grants, consulting, advisory board, speaker’s bureau – Gilead Sciences; research grants – Abbvie; speaker’s bureau – Salix, Bayer; research grant – AASLD Foundation; Tram Tran: employee and stocks – Gilead Sciences; Harvey Kaufman: None; Justin Niles: None; Robert Gish: consulting, advisor - Abbot, AbbVie, Alexion, Arrowhead, Bayer AG, Biocollections, Bristol-Myers Squibb Company, Contravir, Eiger, Enyo, eStudySite, Genentech, Gilead Sciences, HepaTX, HepQuant, Hoffmann-LaRoche Ltd., Intellia, Intercept, Ionis Pharmaceuticals, Janssen, MedImmune, Merck, Prometheus, Quest, Shionogi, Transgene, Trimaran; Scientific/clinical Advisory Boards -AbbVie, Merck, Arrowhead, Bayer, Contravir, Dova Pharmaceuticals, Eiger, Enyo, Janssen, Medimmune, Janssen/J&J, Intercept, Shionogi, Spring Bank; Clinical trials – eStudySite. Chair Clinical Advisory Board – Arrowhead; Data Safety Monitoring Board – Ionis; Speaker’s bureau – AbbVie, Alexion, Bayer, BMS, Gilead Sciences Inc., Merck; Minor stock shareholder - Athenex, Triact, Synageva, RiboSciences, CoCrystal; Stock options – Arrowhead, Eiger. The above competing interests statement and funding do not alter our adherence to all PLOS ONE policies on sharing data and materials.
Figures
References
-
- Wong RJ, Aguilar M, Cheung R, Perumpail RB, Harrison SA, Younossi ZM, et al. Nonalcoholic steatohepatitis is the second leading etiology of liver disease among adults awaiting liver transplantation in the United States. Gastroenterology. 2015;148(3):547–55. 10.1053/j.gastro.2014.11.039 . - DOI - PubMed
-
- Goldberg D, Ditah IC, Saeian K, Lalehzari M, Aronsohn A, Gorospe EC, et al. Changes in the Prevalence of Hepatitis C Virus Infection, Nonalcoholic Steatohepatitis, and Alcoholic Liver Disease Among Patients With Cirrhosis or Liver Failure on the Waitlist for Liver Transplantation. Gastroenterology. 2017;152(5):1090–9 e1. 10.1053/j.gastro.2017.01.003 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
