

The routes of infection spread in central skull-base osteomyelitis and the diagnostic role of CT and MRI scans
- PMID: 31370785
- PMCID: PMC6676590
- DOI: 10.1186/s12880-019-0331-7
The routes of infection spread in central skull-base osteomyelitis and the diagnostic role of CT and MRI scans
Abstract
Background: Central skull-base osteomyelitis (CSBO) represents a life-threatening complication of external ear canal infection. Computed tomography (CT) and magnetic resonance imaging (MRI) play key roles in assessment of CSBO progression.
Methods: Twelve patients with CSBO were included in a retrospective clinical study. In total, 62 scans (30 CTs and 32 MRIs) were performed to evaluate the extent of inflammatory changes. The scans were read independently by two radiologists specialised in imaging of the head and neck. The regions under the skull base were specified using the online Anatomy Atlas of the skull base. To clarify the timeline, the time period was divided into four parts, and inflammatory changes in the skull-base regions were tracked. Data were statistically analysed.
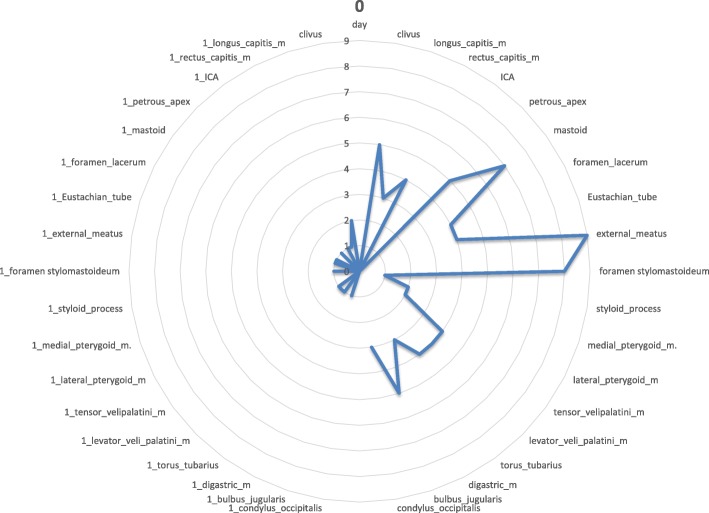
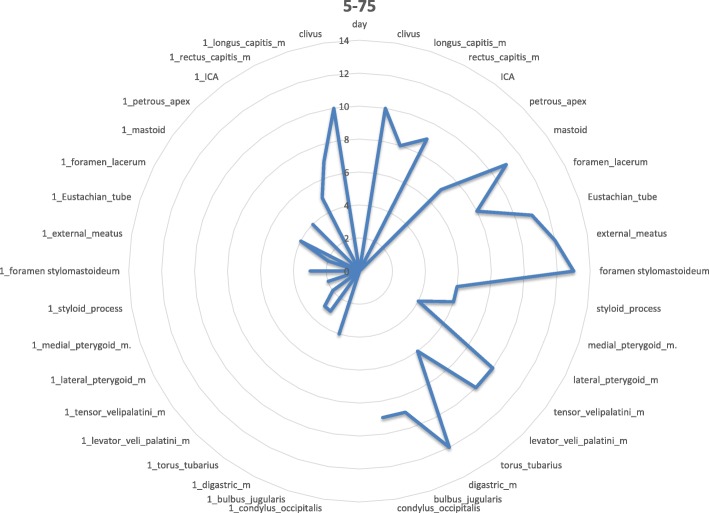
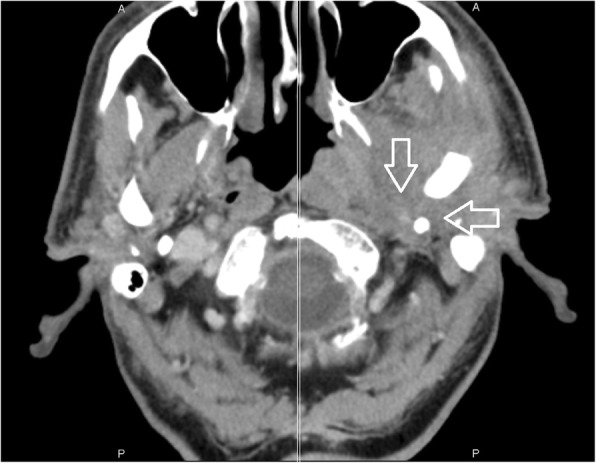
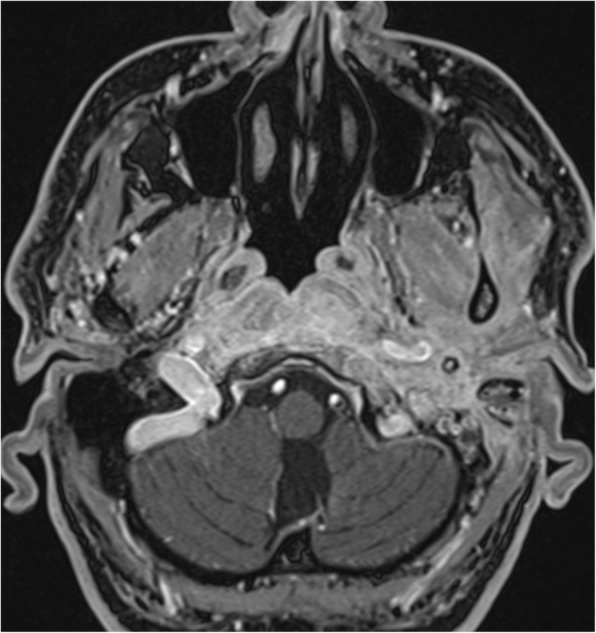
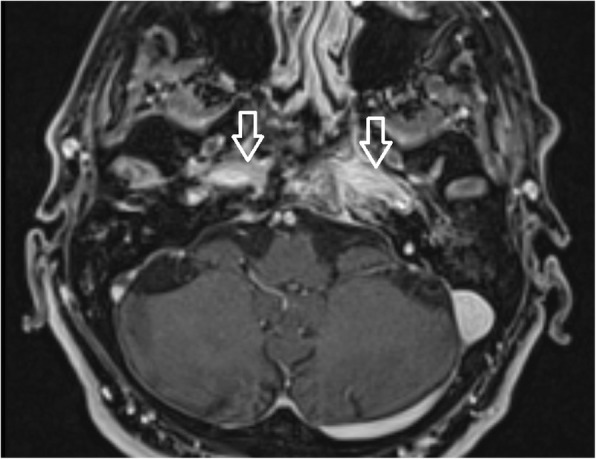
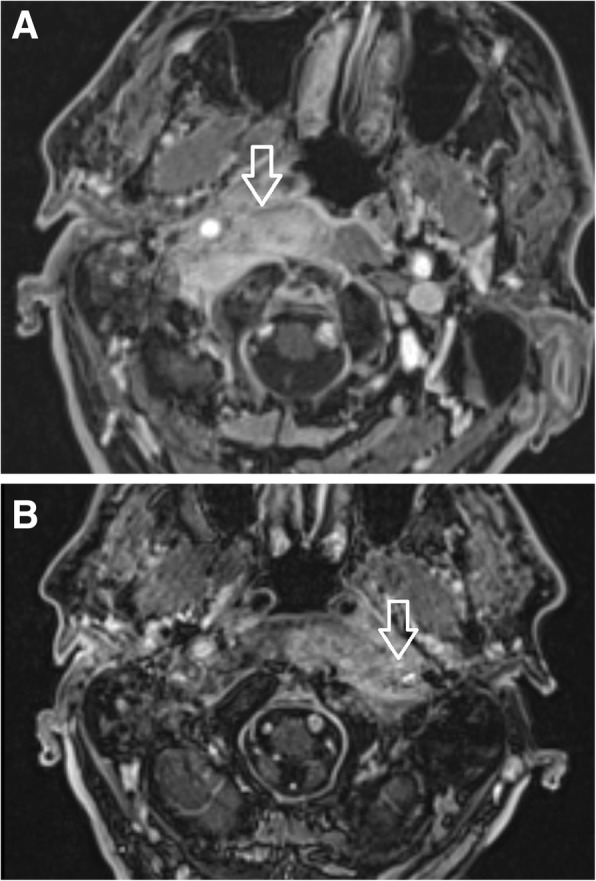
Results: In early stages of the disease, CT scan detects inflammatory changes closely related to the stylomastoid foramen and medially to the posterior belly of the digastric muscle, changes which have been proved to be crucial for the diagnosis of CSBO. Later the infection spreads to the contralateral side causing demineralisation of the bones.
Conclusion: Imaging methods play a crucial role not only in establishing the diagnosis, but also in anticipating the direction of infection spread underneath the skull base.
Keywords: Central skull-base osteomyelitis; Cranial nerve palsy, computed tomography; Imaging; Treatment.
Conflict of interest statement
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Figures





References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
