

National Trends in Healthcare-Associated Infections for Five Common Cardiovascular Conditions
- PMID: 31371062
- PMCID: PMC7883647
- DOI: 10.1016/j.amjcard.2019.06.029
National Trends in Healthcare-Associated Infections for Five Common Cardiovascular Conditions
Abstract
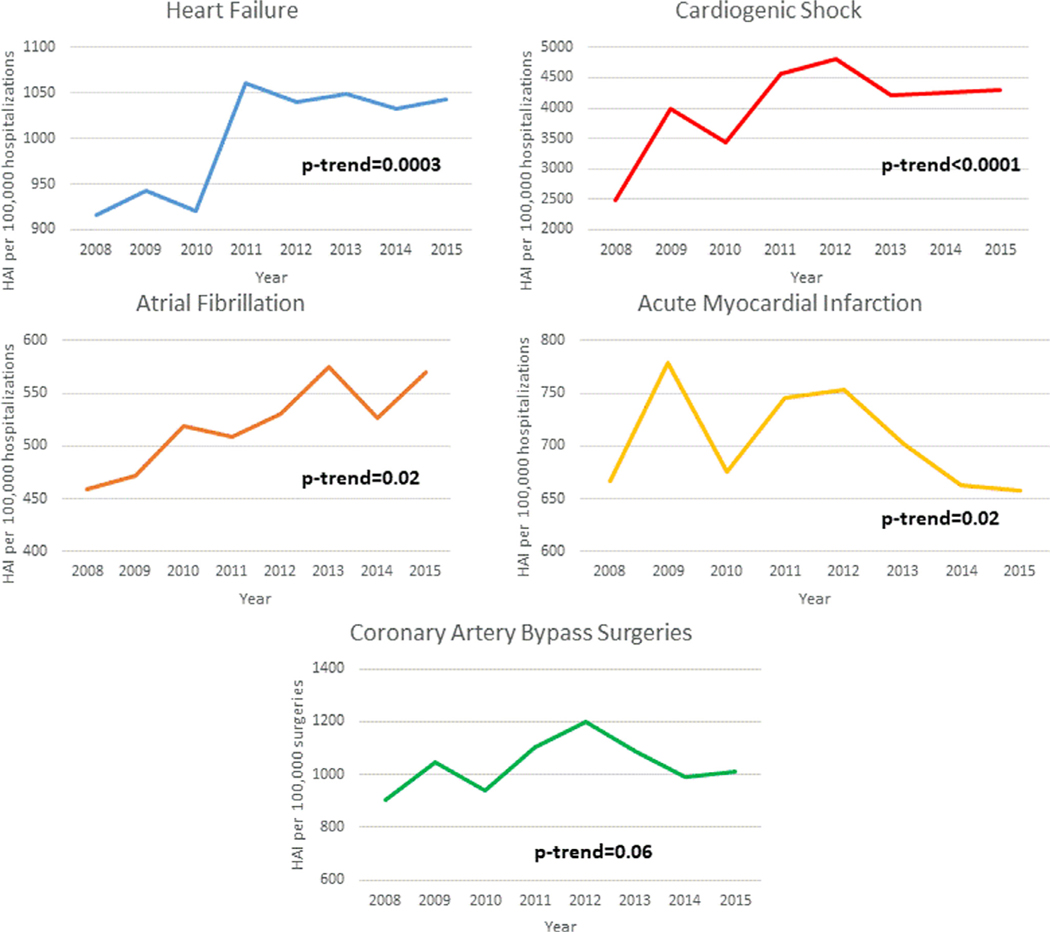
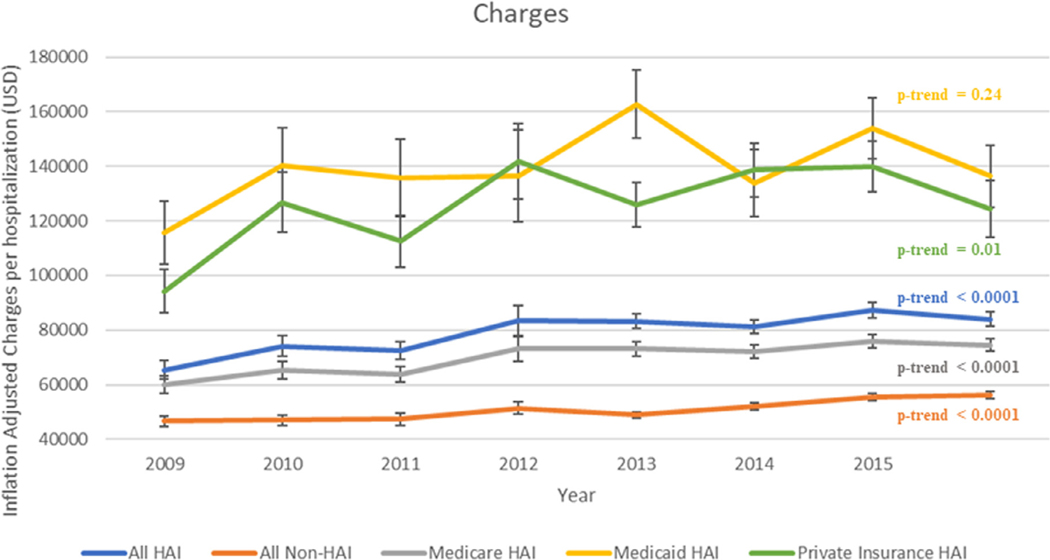
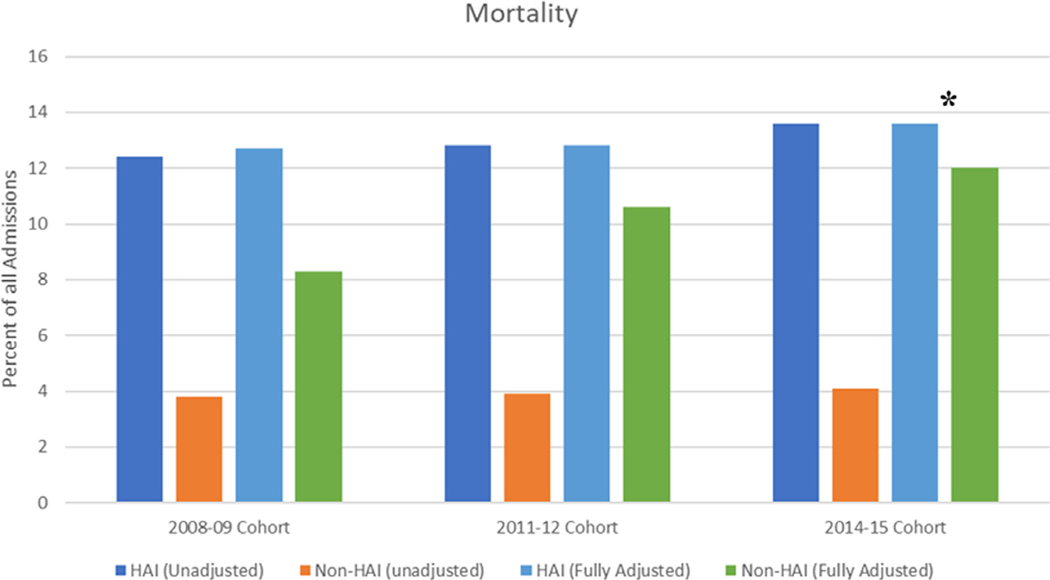
Healthcare-associated infections (HAI) are generally preventable causes of increased cost, morbidity, and mortality. Further, HAI carry penalties in the era of hospital value-based care. However, very little is known about the incidence and outcomes of HAI among patients hospitalized with common cardiovascular conditions. Using a national database, we identified adults aged ≥18 years hospitalized with 5 common cardiovascular conditions, including heart failure, acute myocardial infarction, coronary artery bypass grafting, cardiogenic shock, and atrial fibrillation or flutter. We assessed for temporal trends in incidence, cost, length of stay (LOS), and mortality associated with ventilator-associated pneumonia, catheter-associated urinary tract infections, central line-associated bloodstream infection, and Clostridium difficile infections. Between 2008 and 2015, we identified 159,021 hospitalizations ≥1 HAI (49.6% heart failure, 20.4% acute myocardial infarction, 10.5% coronary artery bypass grafting, 18.6% cardiogenic shock, and 11.9% atrial fibrillation or flutter). Clostridium difficile infections (75.4%) were the most common followed by catheter-associated urinary tract infections (15.1%), ventilator-associated pneumonia (7.9%), and central line-associated bloodstream infection (3.1%). Nearly half of the patients (46.3%) with HAI required discharge to a skilled care facility compared with 15.7% of patients who did not. After propensity matching, HAI remained associated with an increased LOS (4.9 vs 9.6 days, p <0.0001), total hospital charges ($79,227 vs $50,699, p <0.0001), and in-hospital mortality (13% vs 10.4%, p <0.0001) compared with patients who did not acquire a HAI. In conclusion, patients with cardiovascular disease acquiring a HAI had substantially higher costs, LOS, and mortality.
Copyright © 2019 Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosures
The authors have no conflicts of interest to disclose.
Figures
References
-
- Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jimenez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Mackey RH, Matsushita K, Mozaffarian D, Mussolino ME, Nasir K, Neumar RW, Palaniappan L, Pandey DK, Thiagarajan RR, Reeves MJ, Ritchey M, Rodriguez CJ, Roth GA, Rosamond WD, Sasson C, Towfighi A, Tsao CW, Turner MB, Virani SS, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P, American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2017 update: a report from the American Heart Association. Circulation 2017;135:e146–e603. - PMC - PubMed
-
- Torio CM, Moore BJ. National inpatient hospital costs: the most expensive conditions by payer, 2013: HCUP Statistical brief #204. May 2016. Agency for Healthcare Research and Quality, Rockville, MD. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
