

The safety and the efficacy of computed tomography guided percutaneous radiofrequency ablation of osteoid osteoma
- PMID: 31371131
- PMCID: PMC6819852
- DOI: 10.1016/j.aott.2019.06.001
The safety and the efficacy of computed tomography guided percutaneous radiofrequency ablation of osteoid osteoma
Abstract
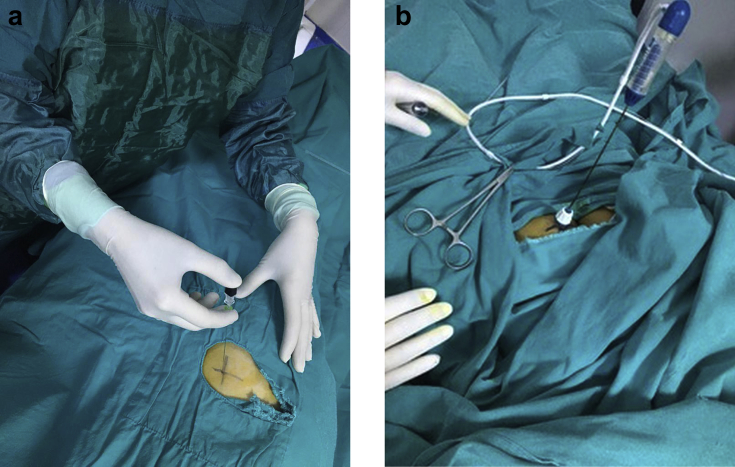
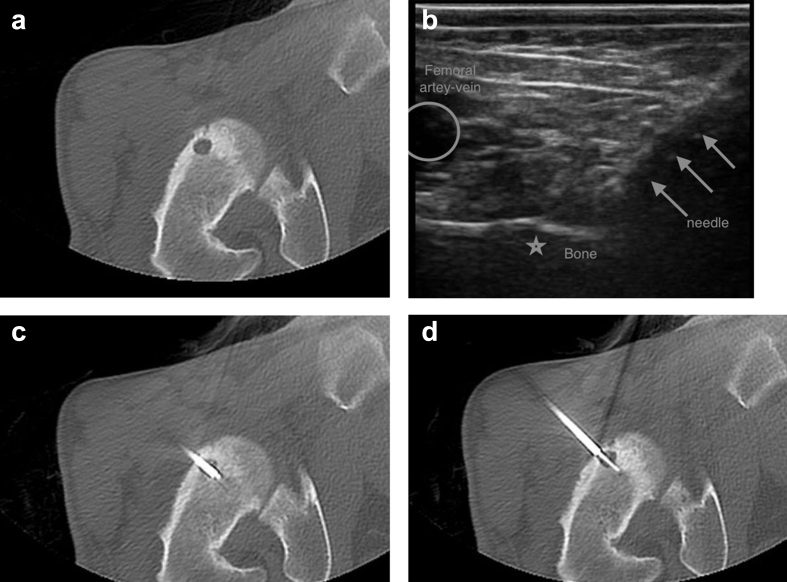
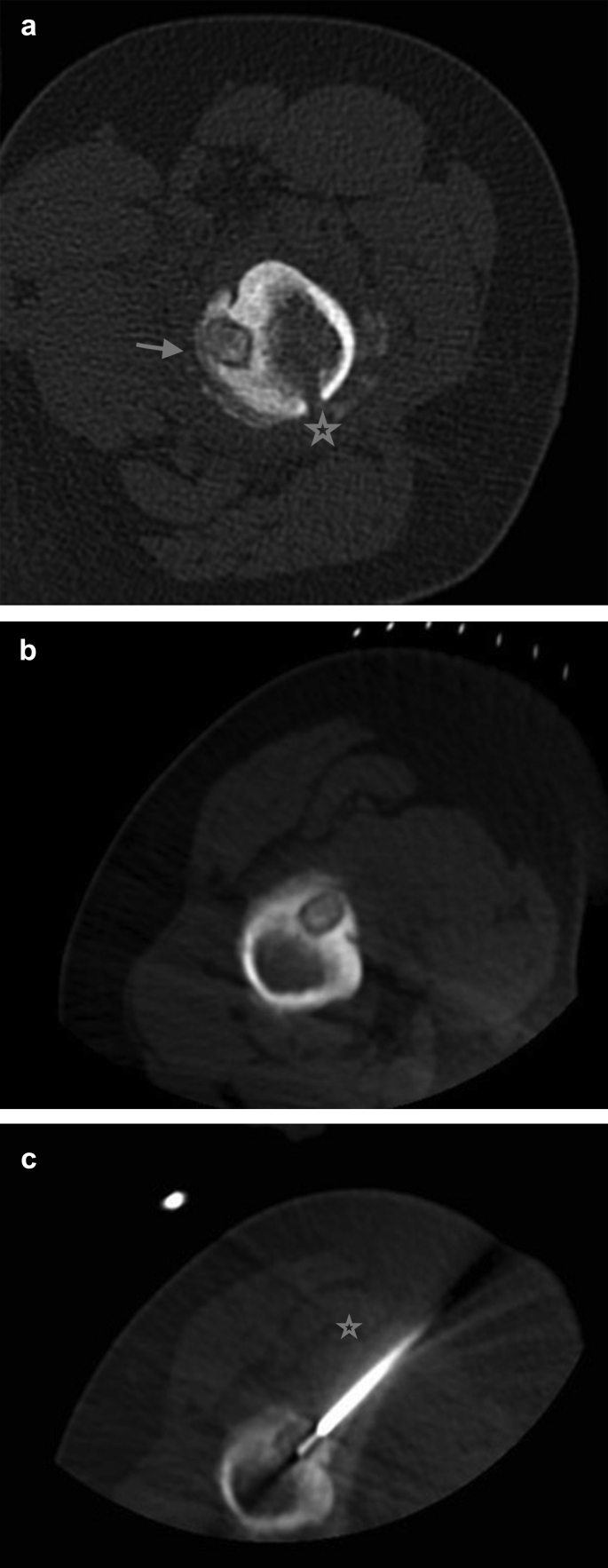
Objective: The aim of this study was to investigate the efficacy and safety of Computed Tomography (CT) guided percutaneous Radiofrequency Ablation (RFA) in the treatment of osteoid osteoma (OO).
Methods: A total of 116 patients (82 male and 34 female patients; mean age of 17.7 years; age range 13-months-42 years) who had 118 CT guided RFA treatment between June 2015 and November 2018 (42 moths) with the diagnosis of OO were included in this study. All the patients had pre-procedural CT examinations. The clinical and technical success and the safety of the treatment were evaluated by assessing the clinical pain symptoms, complication rates and recovery of posture and gait.
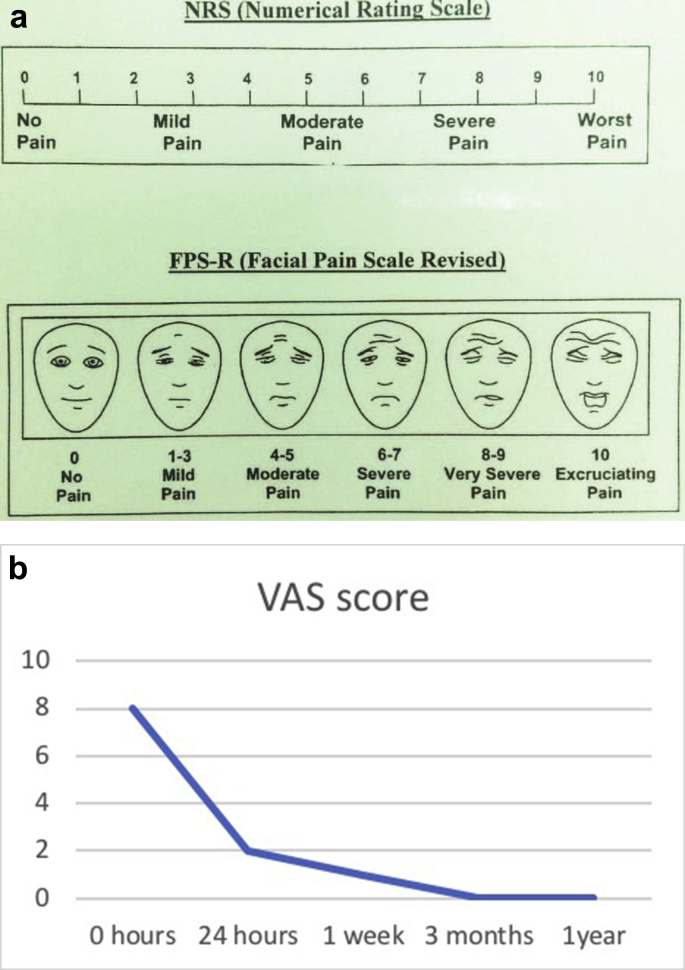
Results: All the patients had a favorable immediate relief of the known pain caused by osteoid osteoma in 24 h after the procedure. Only in two patients (15-years-old boy with OO in right femoral neck and a 12 years old boy with OO in femur diaphysis) pain relapse was occurred in 3 months and 12 months after RFA and a second RFA was performed. During follow-up they had no pain. The technical success and efficacy-rates of the procedure were recorded as 100% and 98% respectively in this study. No significant complication was observed during treatment or recovery period. Seven minor complications were noted which were successfully treated.
Conclusion: The rapid relief of pain symptoms, low relapse rate and low complication rates demonstrate the efficacy and safety of RFA therapy. RFA is an out-patient procedure that patients can be mobilized immediately after the procedure. RFA can be safely used as a first choice of treatment method in OO therapy.
Level of evidence: Level IV, therapeutic study.
Keywords: Efficacy; Osteoid osteoma; Radio frequency ablation; Safety; Treatment.
Copyright © 2019 Turkish Association of Orthopaedics and Traumatology. Production and hosting by Elsevier B.V. All rights reserved.
Figures

Similar articles
-
Our Single Center Experience in Osteoid Osteoma Patients Treated with CTGuided Percutaneous Radiofrequency Ablation Treatment and Follow-up.Curr Med Imaging. 2024;20:e270623218293. doi: 10.2174/1573405620666230627095757. Curr Med Imaging. 2024. PMID: 37366354
-
Therapeutic outcome of CT-guided radiofrequency ablation in patients with osteoid osteoma.Skeletal Radiol. 2017 Jul;46(7):949-956. doi: 10.1007/s00256-017-2658-x. Epub 2017 Apr 20. Skeletal Radiol. 2017. PMID: 28429047
-
[CT-guided radiofrequency ablation for osteoid osteoma].Fukuoka Igaku Zasshi. 2008 Oct;99(10):214-7. Fukuoka Igaku Zasshi. 2008. PMID: 19195219 Japanese.
-
CT-guided radiofrequency ablation for osteoid osteomas: a systematic review.Eur Radiol. 2020 Nov;30(11):5952-5963. doi: 10.1007/s00330-020-06970-y. Epub 2020 Jun 9. Eur Radiol. 2020. PMID: 32518986 Free PMC article.
-
CT-guided radiofrequency ablation of osteoid osteoma: established concepts and new ideas.Br J Radiol. 2020 Oct 1;93(1114):20200266. doi: 10.1259/bjr.20200266. Epub 2020 Jun 24. Br J Radiol. 2020. PMID: 32520586 Free PMC article. Review.
Cited by
-
CT-guided radiofrequency ablation of painful intra-articular osteoid osteoma in children: Is there a concern for cartilage damage?Radiol Med. 2023 Aug;128(8):999-1006. doi: 10.1007/s11547-023-01661-2. Epub 2023 Jun 21. Radiol Med. 2023. PMID: 37341845
-
[Percutaneous radiofrequency ablation of osteoid osteoma: results from 9 years of experience in a third-level center.].Rev Fac Cien Med Univ Nac Cordoba. 2024 Jun 28;81(2):336-352. doi: 10.31053/1853.0605.v81.n2.42451. Rev Fac Cien Med Univ Nac Cordoba. 2024. PMID: 38941221 Free PMC article. Spanish.
-
Osteoid osteoma: which is the best mininvasive treatment option?Eur J Orthop Surg Traumatol. 2021 Dec;31(8):1611-1624. doi: 10.1007/s00590-021-02946-w. Epub 2021 Apr 11. Eur J Orthop Surg Traumatol. 2021. PMID: 33839926 Free PMC article. Review.
-
Secondary radiological findings of osteoid osteoma as muscular atrophy and synovitis in paediatric and adult patients.Pol J Radiol. 2020 Jun 22;85:e316-e322. doi: 10.5114/pjr.2020.97007. eCollection 2020. Pol J Radiol. 2020. PMID: 32685067 Free PMC article.
-
Osteoid Osteoma in an Adult Wheelchair Basketball Player Mimicking Musculoskeletal Shoulder Pain: Red Flag or a Red Herring?Tomography. 2022 Feb 7;8(1):389-401. doi: 10.3390/tomography8010032. Tomography. 2022. PMID: 35202197 Free PMC article.
References
-
- Iyer R.S., Chapman T., Chew F.S. Pediatric bone imaging: diagnostic imaging of osteoid osteoma. AJR. 2012;198(5):1039–1052. - PubMed
-
- Rosenthal D.I., Springfield D.S., Gebhardt M.C., Rosenberg A.E., Mankin H.J. Osteoid osteoma: percutaneous radio-frequency ablation. Radiology. 1995;197(2):451–454. - PubMed
-
- Rosenthal D.I., Hornicek F.J., Wolfe M.W. Percutaneous radiofrequency coagulation of osteoid osteoma compared with operative treatment. J Bone Joint Surg Am. 1998;80(6):815–821. - PubMed
-
- Rosenthal D.I., Ouellette H. Radiofrequency ablation of osteoid osteoma. In: vanSonnenberg E., McMullen W.N., Solbiati L., Livraghi T., Müeller P.R., Silverman S.G., editors. Tumor Ablation. Springer; New York: 2005. pp. 389–401.
-
- Parlier-Cuau C., Nizard R., Champsaur P., Hamze B., Quillard A., Laredo J.D. Osteoid osteoma of the acetabulum. Three cases treated by percutaneous resection. Clin Orthop Relat Res. 1999;365:167–174. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
