

FGFR1 Amplification Mediates Endocrine Resistance but Retains TORC Sensitivity in Metastatic Hormone Receptor-Positive (HR+) Breast Cancer
- PMID: 31371343
- PMCID: PMC6825550
- DOI: 10.1158/1078-0432.CCR-19-0138
FGFR1 Amplification Mediates Endocrine Resistance but Retains TORC Sensitivity in Metastatic Hormone Receptor-Positive (HR+) Breast Cancer
Abstract
Purpose: While FGFR1 amplification has been described in breast cancer, the optimal treatment approach for FGFR1-amplified (FGFR1+) metastatic breast cancer (MBC) remains undefined.Experimental Design: We evaluated clinical response to endocrine and targeted therapies in a cohort of patients with hormone receptor-positive (HR+)/HER2- MBC and validated the functional role of FGFR1-amplification in mediating response/resistance to hormone therapy in vitro.
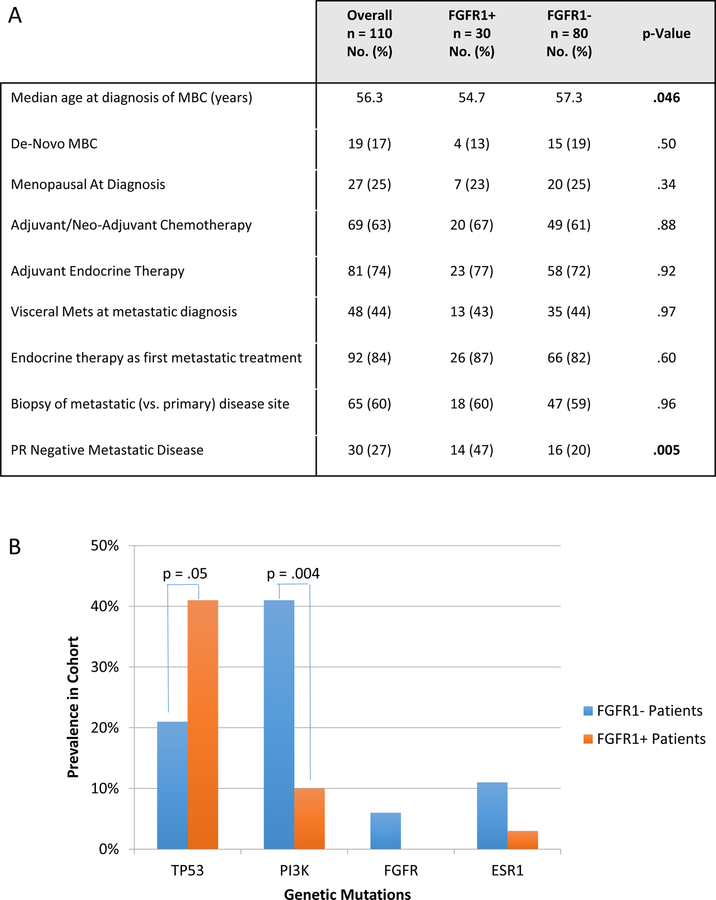
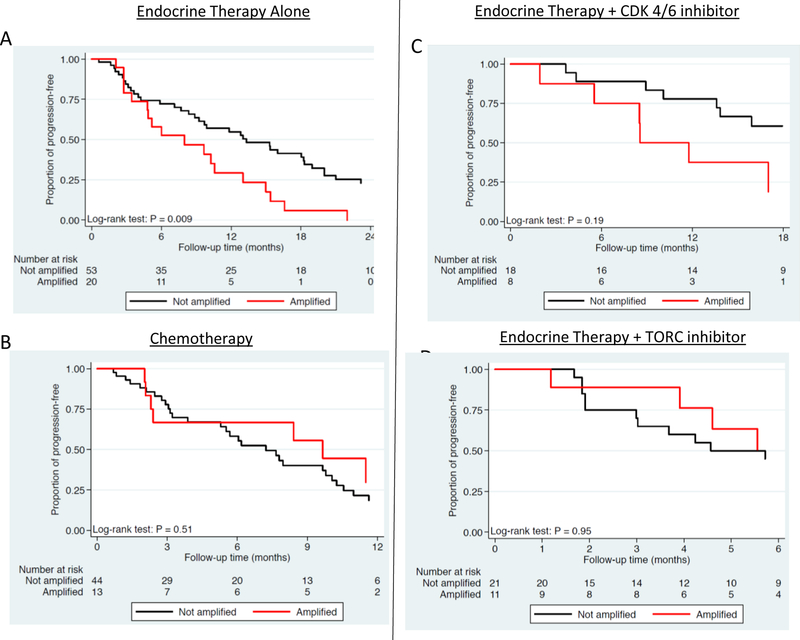
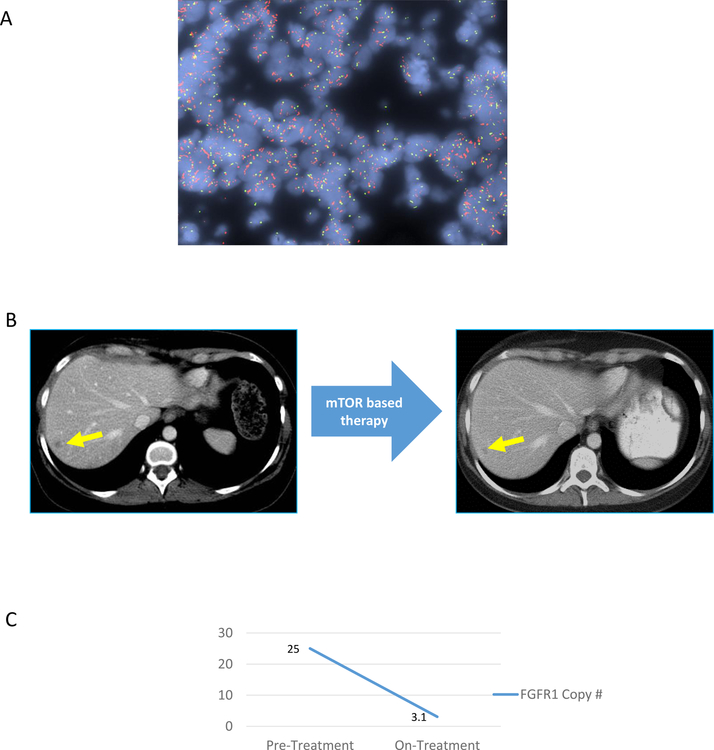
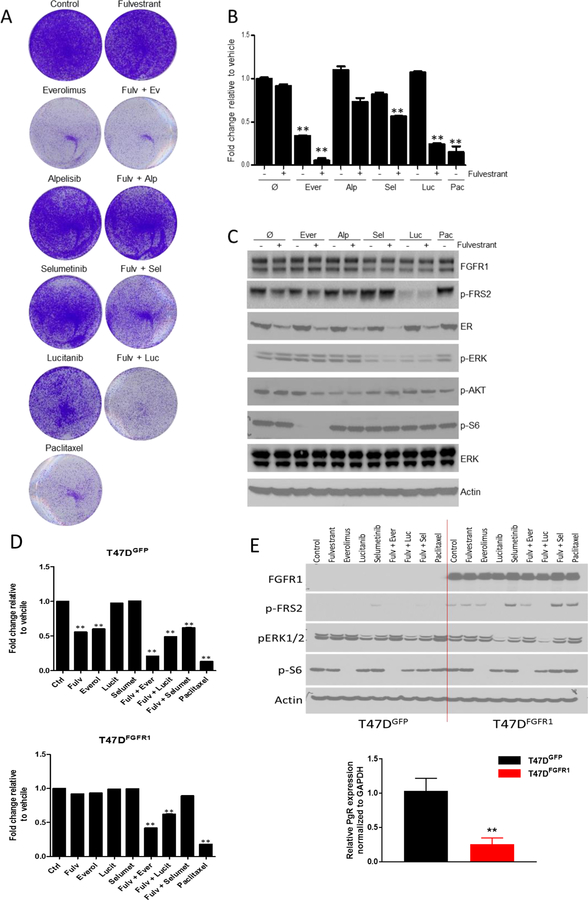
Results: In the clinical cohort (N = 110), we identified that patients with FGFR1+ tumors were more likely to have progesterone receptor (PR)-negative disease (47% vs. 20%; P = 0.005), coexisting TP53 mutations (41% vs. 21%; P = 0.05), and exhibited shorter time to progression with endocrine therapy alone and in combination with CDK4/6 inhibitor, but not with a mTOR inhibitor (everolimus), adjusting for key prognostic variables in multivariate analysis. Furthermore, mTOR-based therapy resulted in a sustained radiological and molecular response in an index case of FGFR1+ HR+/HER2- MBC. In preclinical models, estrogen receptor-positive (ER+)/FGFR1-amplified CAMA1 human breast cancer cells were only partially sensitive to fulvestrant, palbociclib, and alpelisib, but highly sensitive to everolimus. In addition, transduction of an FGFR1 expression vector into ER+ T47D cells induced resistance to fulvestrant that could be overcome by added TORC1 inhibition, but not PI3K or CDK4/6 inhibition.
Conclusions: Collectively, these findings suggest that while FGFR1 amplification confers broad resistance to ER, PI3K, and CDK4/6 inhibitors, mTOR inhibitors might have a unique therapeutic role in the treatment of patients with ER+/FGFR1+ MBC.
©2019 American Association for Cancer Research.
Conflict of interest statement
Conflict of Interest disclosure:
DJ: Consultant/advisory board: Novartis, Genentech, Eisai, Ipsen, EMD Serono.
LF: Grant Support: Lilly.
LS: Consultant/advisory board: Novartis.
DS: Ownership interests and Intellectual property rights/inventor/patent holder: Biotheronostics.
SJI: Consultant/advisory board: Abbvie, PharaMar, Genentech/Roche, Myriad Genetics, Hengrui Therapuetics, Puma Biotech, Immunomedics.
BM: Consultant/advisory board: MOTUS GI (spouse).
AJI: Consultant/advisory board: Roche, Chugai, Constellation, Pfizer. Ownership interests and Intellectual property rights/inventor/patent holder: ArcherDx.
CLA: Stock options: Provista, Y-Trap; Advisory Roles: Symphogen, Daiichi Sankyo, Taiho Oncology, PUMA Biotechnology, Novartis, Merck, Lilly, Radius, Sanofi, H3Biomedicine, OrigiMed. Grant Support: Pfizer, Lilly, Radius.
AB: Consultant/advisory board: Novartis, Pfizer, Genentech/Roche, Radius Health, Merck, Spectrum pharma, Immunomedics, Taiho Oncology, Sanofi, Diiachi, Puma. Research Grant (self): Biothernostics. Research Grant (institution): Novartis, Pfizer, Genentech/Roche, Radius Health, Merck, Immunomedics, Sanofi.
Figures
Similar articles
-
Aberrant FGFR signaling mediates resistance to CDK4/6 inhibitors in ER+ breast cancer.Nat Commun. 2019 Mar 26;10(1):1373. doi: 10.1038/s41467-019-09068-2. Nat Commun. 2019. PMID: 30914635 Free PMC article.
-
Circulating Tumor DNA Markers for Early Progression on Fulvestrant With or Without Palbociclib in ER+ Advanced Breast Cancer.J Natl Cancer Inst. 2021 Mar 1;113(3):309-317. doi: 10.1093/jnci/djaa087. J Natl Cancer Inst. 2021. PMID: 32940689 Free PMC article.
-
Effective combination therapies in preclinical endocrine resistant breast cancer models harboring ER mutations.Oncotarget. 2016 Aug 23;7(34):54120-54136. doi: 10.18632/oncotarget.10852. Oncotarget. 2016. PMID: 27472462 Free PMC article.
-
Sequencing Endocrine Therapy for Metastatic Breast Cancer: What Do We Do After Disease Progression on a CDK4/6 Inhibitor?Curr Oncol Rep. 2020 May 16;22(6):57. doi: 10.1007/s11912-020-00917-8. Curr Oncol Rep. 2020. PMID: 32415339 Review.
-
Everolimus versus alpelisib in advanced hormone receptor-positive HER2-negative breast cancer: targeting different nodes of the PI3K/AKT/mTORC1 pathway with different clinical implications.Breast Cancer Res. 2020 Apr 6;22(1):33. doi: 10.1186/s13058-020-01271-0. Breast Cancer Res. 2020. PMID: 32252811 Free PMC article. Review.
Cited by
-
Fibroblast growth factor receptor signaling in estrogen receptor-positive breast cancer: mechanisms and role in endocrine resistance.Front Oncol. 2024 Jul 8;14:1406951. doi: 10.3389/fonc.2024.1406951. eCollection 2024. Front Oncol. 2024. PMID: 39040443 Free PMC article. Review.
-
Mechanisms of Resistance to Chemotherapy in Breast Cancer and Possible Targets in Drug Delivery Systems.Pharmaceutics. 2020 Dec 9;12(12):1193. doi: 10.3390/pharmaceutics12121193. Pharmaceutics. 2020. PMID: 33316872 Free PMC article. Review.
-
Nuclear FGFR1 Regulates Gene Transcription and Promotes Antiestrogen Resistance in ER+ Breast Cancer.Clin Cancer Res. 2021 Aug 1;27(15):4379-4396. doi: 10.1158/1078-0432.CCR-20-3905. Epub 2021 May 19. Clin Cancer Res. 2021. PMID: 34011560 Free PMC article.
-
Therapy for Hormone Receptor-Positive, Human Epidermal Growth Receptor 2-Negative Metastatic Breast Cancer Following Treatment Progression via CDK4/6 Inhibitors: A Literature Review.Breast Cancer (Dove Med Press). 2024 Apr 10;16:181-197. doi: 10.2147/BCTT.S438366. eCollection 2024. Breast Cancer (Dove Med Press). 2024. PMID: 38617842 Free PMC article. Review.
-
FGFR4 in endocrine resistance: overexpression and estrogen regulation without direct causative role.Breast Cancer Res Treat. 2025 Jun;211(2):501-515. doi: 10.1007/s10549-025-07666-x. Epub 2025 Mar 17. Breast Cancer Res Treat. 2025. PMID: 40097769
References
-
- Harvey Jennet M., et al. “Estrogen receptor status by immunohistochemistry is superior to the ligand-binding assay for predicting response to adjuvant endocrine therapy in breast cancer.” Journal of clinical oncology 175 (1999): 1474–1474. - PubMed
-
- Musgrove Elizabeth A., and Sutherland Robert L.. “Biological determinants of endocrine resistance in breast cancer.” Nature reviews. Cancer 99 (2009): 631. - PubMed
-
- Johnson Daniel E., and Williams Lewis T.. “Structural and functional diversity in the FGF receptor multigene family.” Advances in cancer research 60 (1992): 1–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
