

Molecular heterogeneity of the cerebriform connective tissue nevus in mosaic overgrowth syndromes
- PMID: 31371346
- PMCID: PMC6672027
- DOI: 10.1101/mcs.a004036
Molecular heterogeneity of the cerebriform connective tissue nevus in mosaic overgrowth syndromes
Abstract
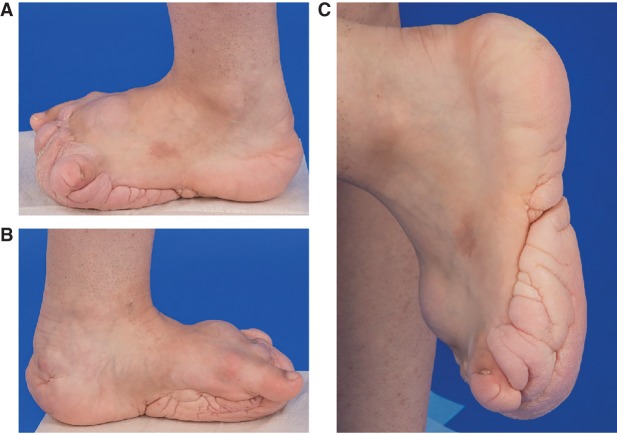
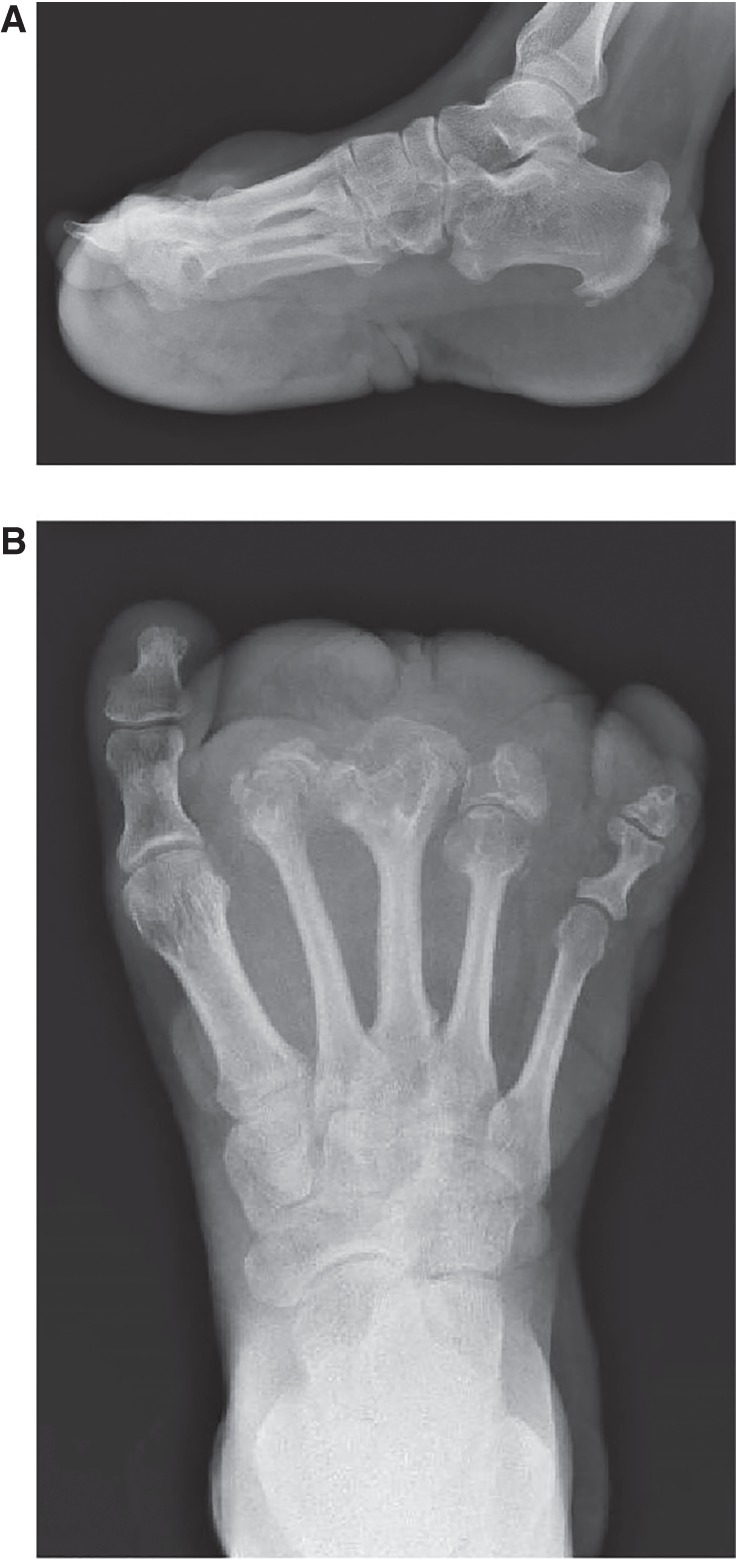
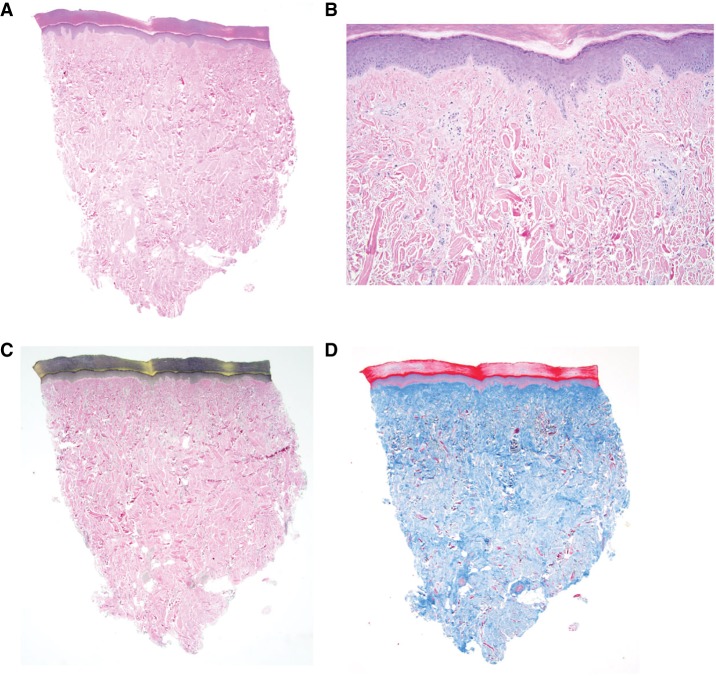
The clinical diagnostic criteria for Proteus syndrome were defined before the discovery of the AKT1 c.49G>A; p.(Glu17Lys) causal variant and used a combination of general and specific phenotypic attributes that could be combined to make a clinical diagnosis. The most heavily weighted specific criterion was the cerebriform connective tissue nevus (CCTN). Here, we describe two individuals with connective tissue nevi (CTNs) and some general attributes of Proteus syndrome who were found to have mosaic PIK3CA variants. CTNs on the soles of individuals with PIK3CA-related overgrowth typically exhibit thickening of the soft tissues with at most a wrinkled surface, but these two patients had firm plaques with ridges and furrows characteristic of CCTNs, which was histologically confirmed in one. These data show that CCTNs are not specific to Proteus syndrome and that clinicians should be cautious in diagnosing individuals with Proteus syndrome based on the CCTN alone. Rather, a complete evaluation should include careful assessment of other attributes of the diagnostic criteria and, whenever possible, genetic analysis of affected tissue.
Keywords: connective tissue nevi; overgrowth.
Published by Cold Spring Harbor Laboratory Press.
Figures



Similar articles
-
Safety findings from the phase 1/2 MOSAIC study of miransertib for patients with PIK3CA-related overgrowth spectrum or Proteus syndrome.Orphanet J Rare Dis. 2025 Jul 25;20(1):375. doi: 10.1186/s13023-025-03831-z. Orphanet J Rare Dis. 2025. PMID: 40713644 Free PMC article. Clinical Trial.
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
The Black Book of Psychotropic Dosing and Monitoring.Psychopharmacol Bull. 2024 Jul 8;54(3):8-59. Psychopharmacol Bull. 2024. PMID: 38993656 Free PMC article. Review.
-
Cyclophosphamide for connective tissue disease-associated interstitial lung disease.Cochrane Database Syst Rev. 2018 Jan 3;1(1):CD010908. doi: 10.1002/14651858.CD010908.pub2. Cochrane Database Syst Rev. 2018. PMID: 29297205 Free PMC article.
Cited by
-
Late-onset Proteus syndrome with cerebriform connective tissue nevus and subsequent development of intraductal papilloma.Am J Med Genet A. 2022 Sep;188(9):2766-2771. doi: 10.1002/ajmg.a.62761. Epub 2022 Apr 20. Am J Med Genet A. 2022. PMID: 35441778 Free PMC article.
-
Phenotype and Surgical Treatment in a Case of Proteus Syndrome With Craniofacial and Oral Findings.In Vivo. 2021 May-Jun;35(3):1583-1594. doi: 10.21873/invivo.12415. In Vivo. 2021. PMID: 33910840 Free PMC article.
References
-
- Biesecker LG. 2005. Proteus syndrome. In Management of genetic syndromes (ed. Cassidy SB, Allanson JE), pp. 449–456. Wiley, New York.
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous