

Autoimmune gait disturbance accompanying adaptor protein-3B2-IgG
- PMID: 31371564
- PMCID: PMC6745733
- DOI: 10.1212/WNL.0000000000008061
Autoimmune gait disturbance accompanying adaptor protein-3B2-IgG
Erratum in
-
Autoimmune gait disturbance accompanying adaptor protein-3B2-IgG.Neurology. 2019 Oct 1;93(14):647. doi: 10.1212/WNL.0000000000008232. Epub 2019 Aug 29. Neurology. 2019. PMID: 31467253 Free PMC article. No abstract available.
Abstract
Objective: To describe phenotypes, treatment response, and outcomes of autoimmunity targeting a synaptic vesicle coat protein, the neuronal (B2) form of adaptor protein-3 (AP3).
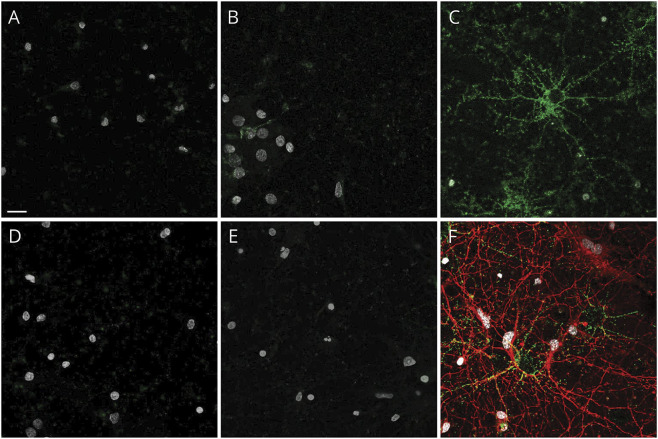
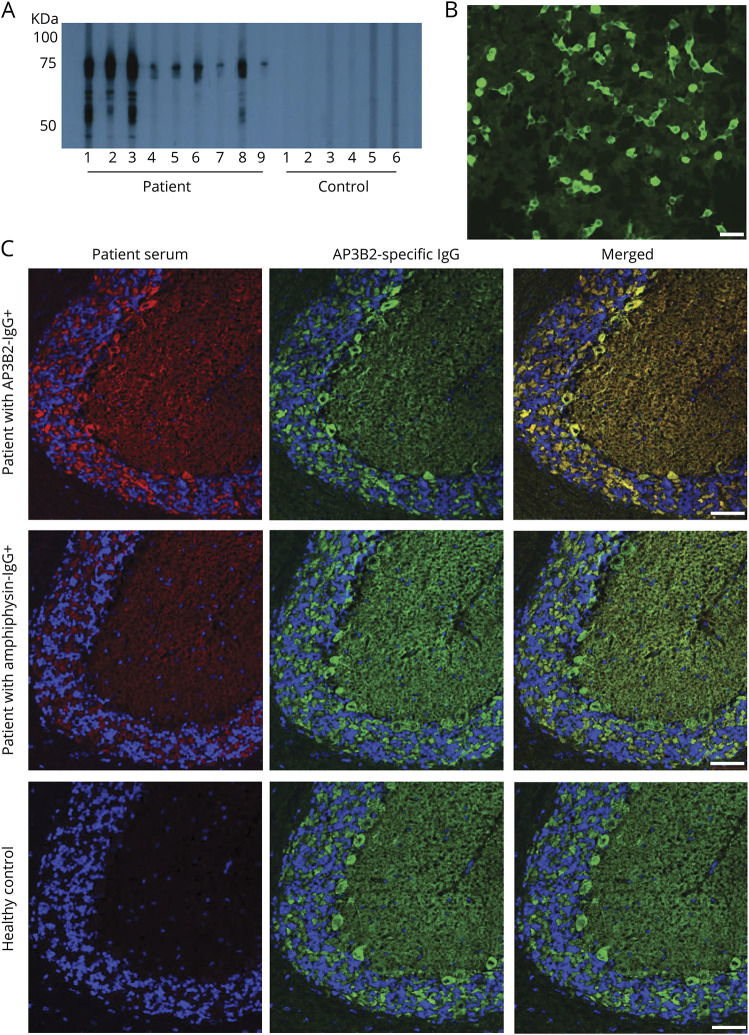
Methods: Archived serum and CSF specimens (from 616,025 screened) harboring unclassified synaptic antibodies mimicking amphiphysin-immunoglobulin G (IgG) on tissue-based indirect immunofluorescence assay (IFA) were re-evaluated for novel IgG staining patterns. Autoantigens were identified by western blot and mass spectrometry. Recombinant western blot and cell-binding assay (CBA) were used to confirm antigen specificity. Clinical data were obtained retrospectively.
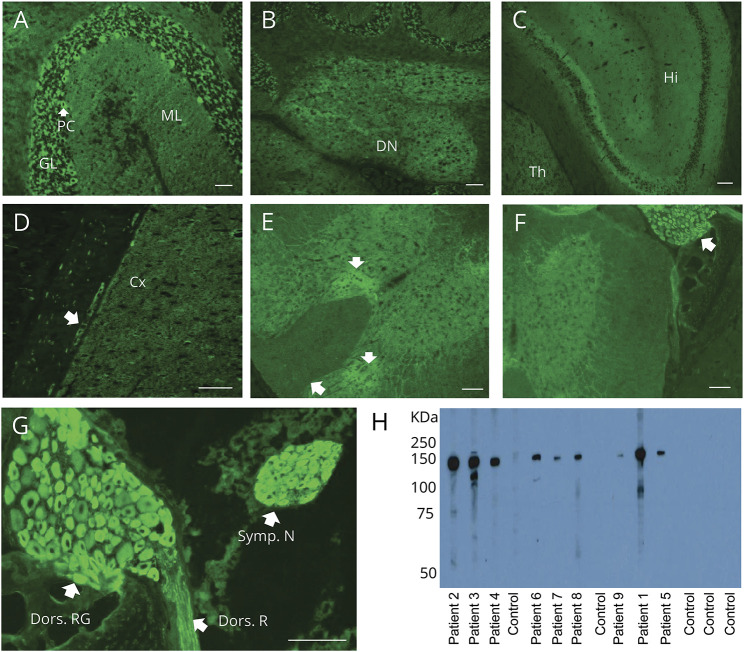
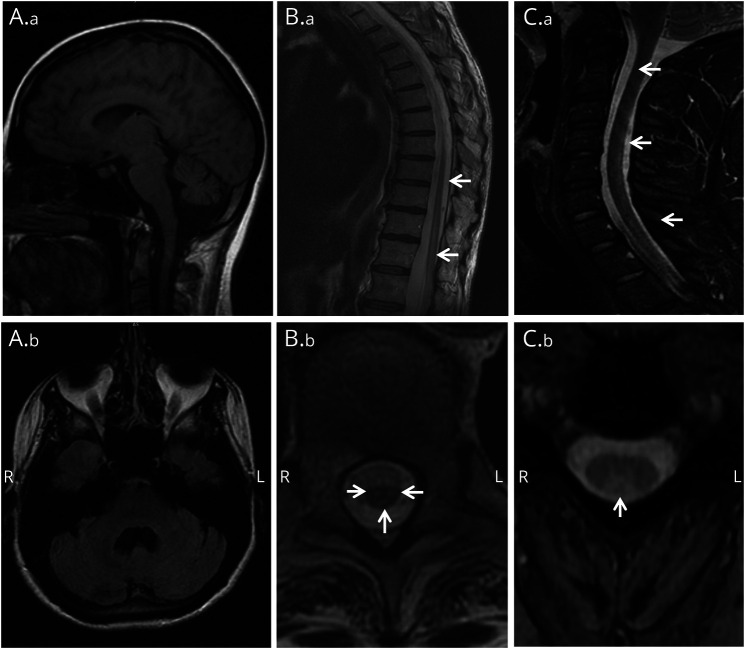
Results: Serum (10) and CSF (6) specimens of 10 patients produced identical IFA staining patterns throughout mouse nervous system tissues, most prominently in cerebellum (Purkinje neuronal perikarya, granular layer synapses, and dentate regions), spinal cord gray matter, dorsal root ganglia, and sympathetic ganglia. The antigen revealed by mass spectrometry analysis and confirmed by recombinant assays (western blot and CBA) was AP3B2 in all. Of 10 seropositive patients, 6 were women; median symptom onset age was 42 years (range 24-58). Clinical information was available for 9 patients, all with subacute onset and rapidly progressive gait ataxia. Neurologic manifestations were myeloneuropathy (3), peripheral sensory neuropathy (2), cerebellar ataxia (2), and spinocerebellar ataxia (2). Five patients received immunotherapy; none improved, but they did not worsen over the follow-up period (median 36 months; range 3-94). Two patients (both with cancer) died. One of 50 control sera was positive by western blot only (but not by IFA or CBA).
Conclusion: AP3B2 (previously named β-neuronal adaptin-like protein) autoimmunity appears rare, is accompanied by ataxia (sensory or cerebellar), and is potentially treatable.
Copyright © 2019 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
-
- McKeon A, Pittock SJ. Paraneoplastic encephalomyelopathies: pathology and mechanisms. Acta Neuropathol 2011;122:381–400. - PubMed
-
- Dalmau J, Graus F, Rosenblum MK, Posner JB. Anti-Hu-associated paraneoplastic encephalomyelitis/sensory neuronopathy: a clinical study of 71 patients. Medicine 1992;71:59–72. - PubMed
-
- Lucchinetti CF, Kimmel DW, Lennon VA. Paraneoplastic and oncologic profiles of patients seropositive for type 1 antineuronal nuclear autoantibodies. Neurology 1998;50:652–657. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases