

Navigation-Assisted Orbital Trauma Reconstruction Using a Bioactive Osteoconductive/Bioresorbable u-HA/PLLA System
- PMID: 31371870
- PMCID: PMC6639503
- DOI: 10.1007/s12663-019-01207-y
Navigation-Assisted Orbital Trauma Reconstruction Using a Bioactive Osteoconductive/Bioresorbable u-HA/PLLA System
Abstract
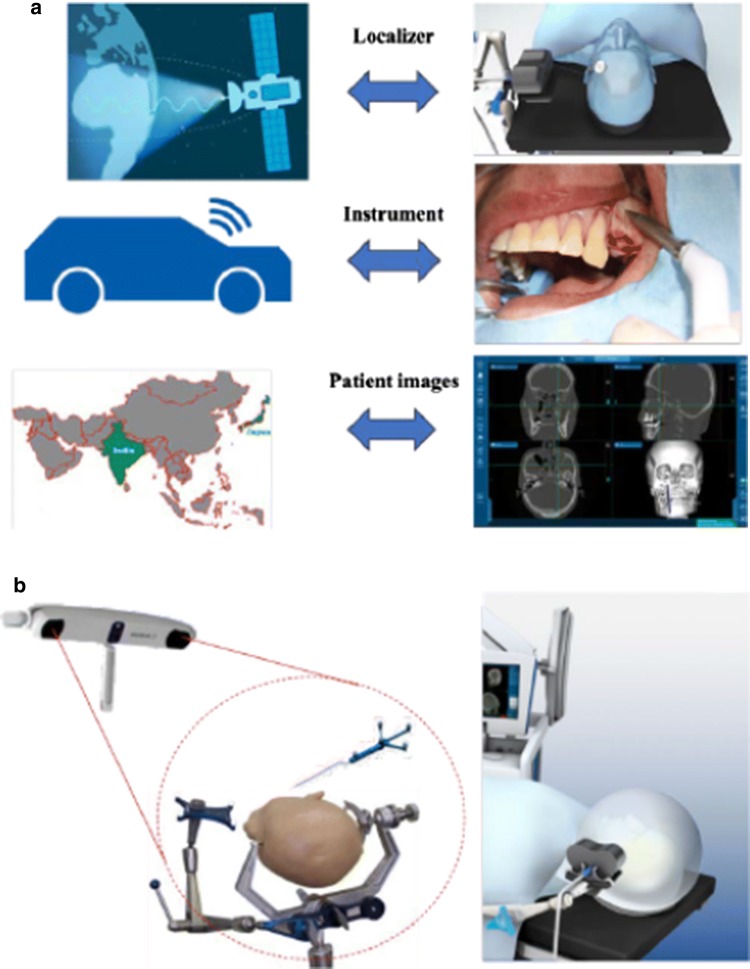
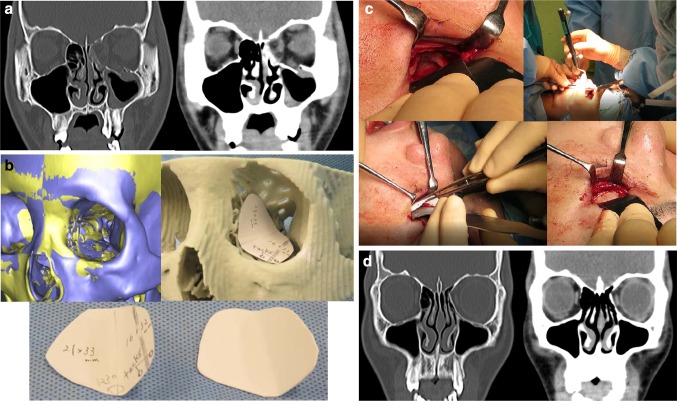
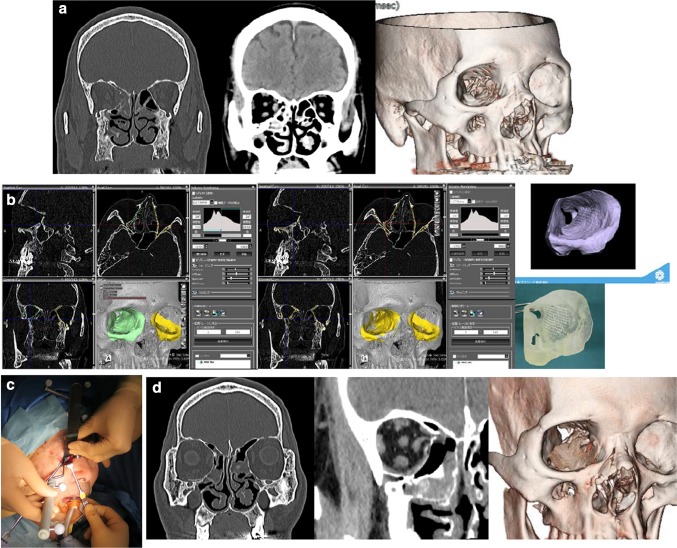
Orbital fractures with orbital wall defects are common facial fractures encountered by oral-maxillofacial surgeons, because of the exposed position and thin bony walls of the midface. The primary goal of surgery is to restore the pre-injury anatomy and volume of hard tissue, and to free incarcerated or prolapsed orbital tissue from the fracture by bridging the bony defects with reconstructive implant material and restoring the maxillofacial-orbital skeleton. Numerous studies have reported orbital fracture repair with a wide variety of implant materials that offer various advantages and disadvantages. The ideal orbital implant material will allow conformation to individual patients' anatomical characteristics, remain stable over time, and are radiopaque, especially for the reconstruction of relatively large and/or complex bony walls. Based on these requirements, novel uncalcined and unsintered hydroxyapatite (u-HA) particles and poly-L-lactide (PLLA; u-HA/PLLA) composite sheets could be used as innovative, bioactive, and osteoconductive/bioresorbable implant materials for orbital reconstruction. In addition, intraoperative navigation is a powerful tool. Navigation- and computer-assisted surgeries have improved execution and predictability, allowing for greater precision, accuracy, and minimal invasiveness during orbital trauma reconstructive surgery of relatively complex and large orbital wall defects with ophthalmological malfunctions and deformities. This review presents an overview of navigation-assisted orbital trauma reconstruction using a bioactive, osteoconductive/bioresorbable u-HA/PLLA system.
Keywords: Navigation; Orbital reconstruction; Orbital trauma; u-HA/PLLA.
Conflict of interest statement
Conflict of interestThe authors declare that there are no conflicts of interest.
Figures

Similar articles
-
Bioactive Regeneration Potential of the Newly Developed Uncalcined/Unsintered Hydroxyapatite and Poly-l-Lactide-Co-Glycolide Biomaterial in Maxillofacial Reconstructive Surgery: An In Vivo Preliminary Study.Materials (Basel). 2021 May 10;14(9):2461. doi: 10.3390/ma14092461. Materials (Basel). 2021. PMID: 34068558 Free PMC article.
-
Immediate and long-term results of unsintered hydroxyapatite and poly L-lactide composite sheets for orbital wall fracture reconstruction.J Plast Reconstr Aesthet Surg. 2018 Jul;71(7):1069-1075. doi: 10.1016/j.bjps.2018.03.006. Epub 2018 Mar 28. J Plast Reconstr Aesthet Surg. 2018. PMID: 29759951
-
A Narrative Review of u-HA/PLLA, a Bioactive Resorbable Reconstruction Material: Applications in Oral and Maxillofacial Surgery.Materials (Basel). 2021 Dec 26;15(1):150. doi: 10.3390/ma15010150. Materials (Basel). 2021. PMID: 35009297 Free PMC article. Review.
-
Bone Regeneration Capacity of Newly Developed Uncalcined/Unsintered Hydroxyapatite and Poly-l-lactide-co-glycolide Sheet in Maxillofacial Surgery: An In Vivo Study.Nanomaterials (Basel). 2020 Dec 24;11(1):22. doi: 10.3390/nano11010022. Nanomaterials (Basel). 2020. PMID: 33374294 Free PMC article.
-
Overview of innovative advances in bioresorbable plate systems for oral and maxillofacial surgery.Jpn Dent Sci Rev. 2018 Aug;54(3):127-138. doi: 10.1016/j.jdsr.2018.03.003. Epub 2018 Apr 5. Jpn Dent Sci Rev. 2018. PMID: 30128060 Free PMC article. Review.
Cited by
-
Comparison between Metal Mesh and Iliac Bonegraft in the Reconstruction of Orbital Floor Fracture-A Clinical Study.J Pharm Bioallied Sci. 2024 Jul;16(Suppl 3):S2637-S2639. doi: 10.4103/jpbs.jpbs_385_24. Epub 2024 Jul 31. J Pharm Bioallied Sci. 2024. PMID: 39346175 Free PMC article.
-
Bone Coverage around Hydroxyapatite/Poly(L-Lactide) Composite Is Determined According to Depth from Cortical Bone Surface in Rabbits.Materials (Basel). 2021 Mar 17;14(6):1458. doi: 10.3390/ma14061458. Materials (Basel). 2021. PMID: 33802655 Free PMC article.
-
Biomechanical Loading Comparison between Titanium and Bioactive Resorbable Screw Systems for Fixation of Intracapsular Condylar Head Fractures.Materials (Basel). 2020 Jul 15;13(14):3153. doi: 10.3390/ma13143153. Materials (Basel). 2020. PMID: 32679803 Free PMC article.
-
Bioactive Regeneration Potential of the Newly Developed Uncalcined/Unsintered Hydroxyapatite and Poly-l-Lactide-Co-Glycolide Biomaterial in Maxillofacial Reconstructive Surgery: An In Vivo Preliminary Study.Materials (Basel). 2021 May 10;14(9):2461. doi: 10.3390/ma14092461. Materials (Basel). 2021. PMID: 34068558 Free PMC article.
-
A retrospective study to compare the treatment outcomes with and without surgical navigation for fracture of the orbital wall.Chin J Traumatol. 2021 Feb;24(1):11-17. doi: 10.1016/j.cjtee.2020.10.002. Epub 2020 Nov 17. Chin J Traumatol. 2021. PMID: 33246880 Free PMC article.
References
-
- Kanno T, Tatsumi H, Karino M, Yoshino A, Koike T, Ide T, Sekine J. Applicability of an unsintered hydroxyapatite particles/poly-L-lactide composite sheet with tack fixation for orbital fracture reconstruction. J Hard Tissue Biol. 2016;25:329–334. doi: 10.2485/jhtb.25.329. - DOI
-
- Sukegawa S, Kanno T, Shibata A, Matsumoto K, Sukegawa-Takahashi Y, Sakaida K, Furuki Y. Treatment of orbital fractures with orbital-wall defects using anatomically preformed orbital wall reconstruction plate system. J Hard Tissue Biol. 2017;26:231–236. doi: 10.2485/jhtb.26.231. - DOI
-
- Gellrich NC, Schramm A, Hammer B, Rojas S, Cufi D, Lagrèze W, Schmelzeisen R. Computer-assisted secondary reconstruction of unilateral posttraumatic orbital deformity. Plast Reconstr Surg. 2002;110:1417–1429. - PubMed
Publication types
LinkOut - more resources
Full Text Sources