

The Difficult Route to Glottis in Cleft Patients Simplified
- PMID: 31371894
- PMCID: PMC6639447
- DOI: 10.1007/s12663-018-1128-x
The Difficult Route to Glottis in Cleft Patients Simplified
Abstract
Introduction: Cleft lip with or without palate is one of the most common craniofacial anomalies worldwide. Airway problems in children with cleft lip and palate were well recognized since very early times.
Objective: The aim of this technical note is to describe a unique method of performing direct laryngoscopy in children with cleft lip and palate by using a palatal obturator to cover the alveolar and palatal defect in these patients.
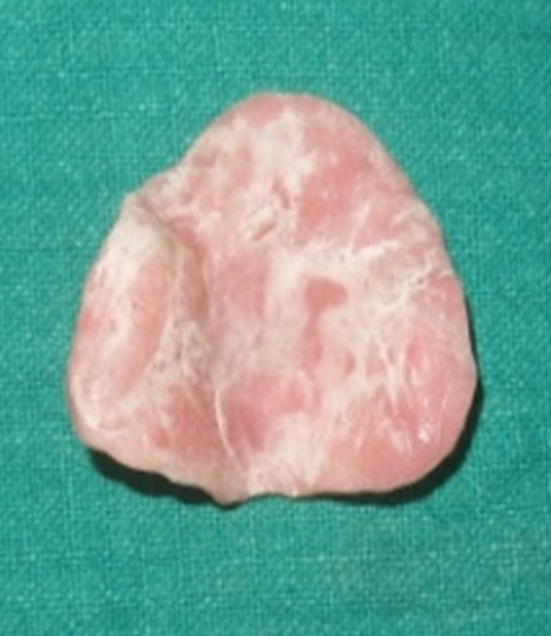
Methods: The palatal obturator was fabricated using cold cure acrylic after making an impression of the defect using putty-type impression material.
Results: The use of the palatal obturator facilitated the placement of the laryngoscope's blade by providing adequate leverage to it during the process of direct laryngoscopy prior to intubating children with cleft lip and palate defect.
Conclusion: A discontinuous alveolar arch and palatal defect contribute to lack of effective leverage of the laryngoscope blade while attempting visualization of the glottis. This difficulty can be overcome by use of an obturator to cover the alveolar and palatal defect in order to provide adequate leverage while using a laryngoscope for visualizing the glottis.
Keywords: Glottis; Intubation; Laryngoscopy.
Conflict of interest statement
Conflict of interestThe author Dr Shyam Bose declares that he has no conflict of interest. The co-author Dr Gunjan Dube declares that he has no conflicts of interest. The co-author Dr. Radhika Shrivastava declares that she has no conflicts of interest. The co-author Dr. Anukool Choube declares that she has no conflicts of interest.
Figures



Similar articles
-
Rehabilitation of a One-day-Old Neonate with Cleft Lip and Palate using Palatal Obturator: A Case Report.Int J Clin Pediatr Dent. 2012 May;5(2):145-7. doi: 10.5005/jp-journals-10005-1154. Epub 2012 Aug 8. Int J Clin Pediatr Dent. 2012. PMID: 25206156 Free PMC article.
-
A new technique of impression making for an obturator in cleft lip and palate patient.J Indian Soc Pedod Prev Dent. 2010 Oct-Dec;28(4):311-4. doi: 10.4103/0970-4388.76165. J Indian Soc Pedod Prev Dent. 2010. PMID: 21273723
-
Feeding obturator as an airway adjunct during complete unilateral cleft palate repair.Indian J Anaesth. 2018 May;62(5):376-380. doi: 10.4103/ija.IJA_714_17. Indian J Anaesth. 2018. PMID: 29910496 Free PMC article.
-
The Impact of Palatal Fistulae on the Success of Alveolar Bone Grafting.J Craniofac Surg. 2021 Mar-Apr 01;32(2):e182-e184. doi: 10.1097/SCS.0000000000007030. J Craniofac Surg. 2021. PMID: 33705068 Review.
-
Role of obturators and other feeding interventions in patients with cleft lip and palate: a review.Eur Arch Paediatr Dent. 2014 Feb;15(1):1-9. doi: 10.1007/s40368-013-0101-0. Epub 2014 Jan 15. Eur Arch Paediatr Dent. 2014. PMID: 24425528 Review.
References
LinkOut - more resources
Full Text Sources