

Effectiveness of low-cost reminder package combined with case-based health education to improve hypertensive patients' medication adherence: a clustered randomized controlled trial
- PMID: 31371926
- PMCID: PMC6628963
- DOI: 10.2147/PPA.S194667
Effectiveness of low-cost reminder package combined with case-based health education to improve hypertensive patients' medication adherence: a clustered randomized controlled trial
Abstract
Purpose: Medication adherence (MA) is a key factor for hypertensive patients' blood pressure control and forgetfulness is one of the main reasons that cause medication non-adherence. If effective, low-cost reminder package (LCRP) has great potentials for large-scale promotion. Therefore, this study aims to evaluate the effectiveness of combining LCRP and health education to improve MA among hypertensive patients.
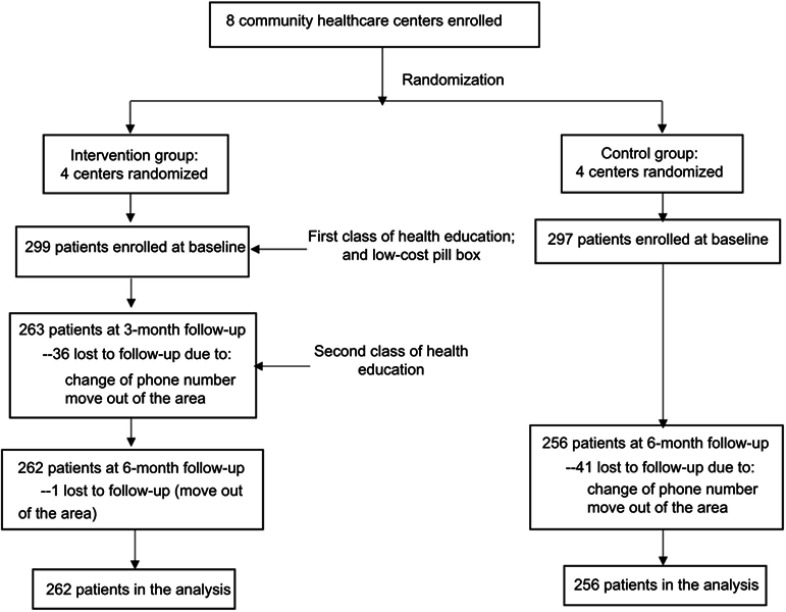
Patients and methods: A clustered randomized controlled trial was performed in Beijing. A total of 518 hypertensive patients recruited from 8 community health care centers were randomized to receive LCRP combined with case-based health education or usual care. Randomization was performed at community level. Multilevel modeling was used to evaluate the study effect.
Results: MA scores did not differ significantly at baseline between the intervention group and the control group. The results of multilevel modeling indicated that MA scores increased more in the intervention group, and the intervention effect on MA was 0.287 (95% CI: [0.103, 0.471], P=0.002). Patients' systolic blood pressure (SBP) and diastolic blood pressure (DBP) were not improved (SBP: difference=0.536, 95% CI [-3.207, 4.278]; DBP: difference=-0.927, 95% CI [-3.283, 1.428]).
Conclusion: LCRP combined with case-based health education could significantly improve hypertensive patients' MA.
Keywords: case-based health education; low-cost reminder package; medication adherence; multilevel modeling.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Similar articles
-
Effectiveness of a Transtheoretical Model-Based Intervention to Improve Blood Pressure Control of Hypertensive Patients in China: A Clustered Randomized Controlled Trial.Front Public Health. 2022 Jan 25;9:760421. doi: 10.3389/fpubh.2021.760421. eCollection 2021. Front Public Health. 2022. PMID: 35145945 Free PMC article. Clinical Trial.
-
Text Messaging to Improve Hypertension Medication Adherence in African Americans From Primary Care and Emergency Department Settings: Results From Two Randomized Feasibility Studies.JMIR Mhealth Uhealth. 2017 Feb 1;5(2):e9. doi: 10.2196/mhealth.6630. JMIR Mhealth Uhealth. 2017. PMID: 28148474 Free PMC article.
-
Culturally adapted hypertension education (CAHE) to improve blood pressure control and treatment adherence in patients of African origin with uncontrolled hypertension: cluster-randomized trial.PLoS One. 2014 Mar 5;9(3):e90103. doi: 10.1371/journal.pone.0090103. eCollection 2014. PLoS One. 2014. PMID: 24598584 Free PMC article. Clinical Trial.
-
A telecommunications system for monitoring and counseling patients with hypertension. Impact on medication adherence and blood pressure control.Am J Hypertens. 1996 Apr;9(4 Pt 1):285-92. doi: 10.1016/0895-7061(95)00353-3. Am J Hypertens. 1996. PMID: 8722429 Clinical Trial.
-
A Systems-Level Approach to Improving Medication Adherence in Hypertensive Latinos: a Randomized Control Trial.J Gen Intern Med. 2020 Jan;35(1):182-189. doi: 10.1007/s11606-019-05419-3. Epub 2019 Oct 17. J Gen Intern Med. 2020. PMID: 31625041 Free PMC article. Clinical Trial.
Cited by
-
A Systematic Review of Compensation and Technology-Mediated Strategies to Maintain Older Adults' Medication Adherence.Int J Environ Res Public Health. 2023 Jan 1;20(1):803. doi: 10.3390/ijerph20010803. Int J Environ Res Public Health. 2023. PMID: 36613130 Free PMC article.
-
Strategies to Improve Adherence to Anti-Hypertensive Medications: a Narrative Review.Curr Hypertens Rep. 2020 Nov 9;22(12):105. doi: 10.1007/s11906-020-01115-4. Curr Hypertens Rep. 2020. PMID: 33165652 Free PMC article. Review.
References
-
- Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the global burden of disease study 2010. The Lancet. 2012;380(9859):2224–2260. doi:10.1016/S0140-6736(12)61766-8 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
