

Active Visceral Manipulation Associated With Conventional Physiotherapy in People With Chronic Low Back Pain and Visceral Dysfunction: A Preliminary, Randomized, Controlled, Double-Blind Clinical Trial
- PMID: 31372099
- PMCID: PMC6656920
- DOI: 10.1016/j.jcm.2018.11.005
Active Visceral Manipulation Associated With Conventional Physiotherapy in People With Chronic Low Back Pain and Visceral Dysfunction: A Preliminary, Randomized, Controlled, Double-Blind Clinical Trial
Abstract
Objective: The purpose of this study was to generate data for conduction of a power analysis to investigate short-term effects of visceral manipulation associated with conventional physical therapy on pain intensity, lumbar mobility, and functionality of people with chronic low back pain and visceral dysfunctions.
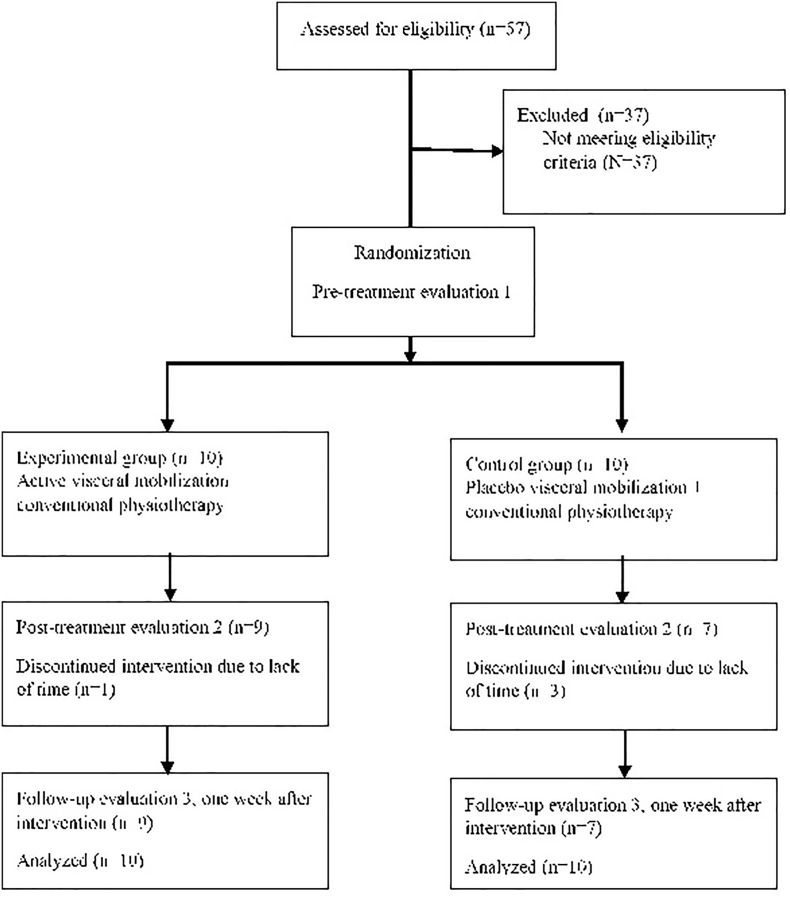
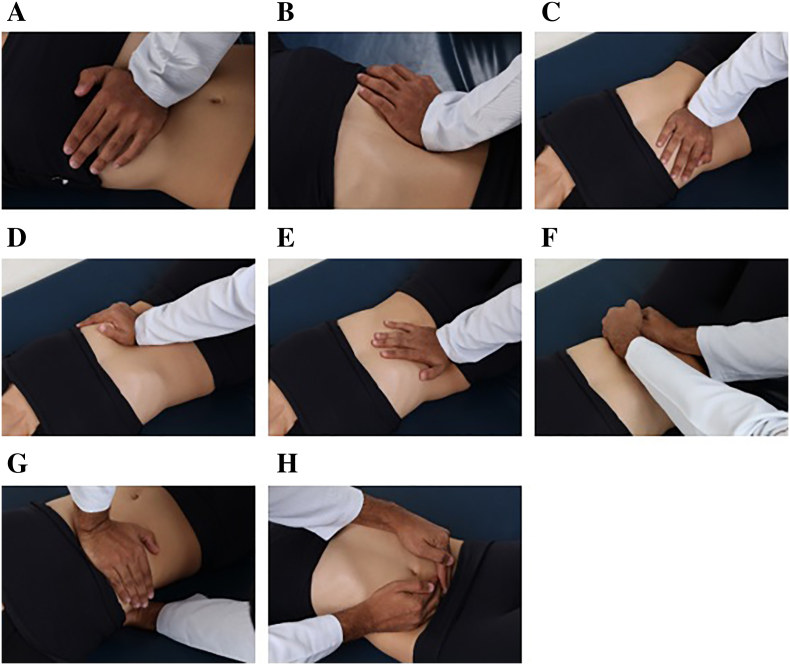
Methods: This was a double-blinded, randomized, controlled, clinical trial preliminary study. A blinded evaluation was conducted involving 20 people with chronic low back pain with visceral dysfunction. Pain perception, lumbar mobility, and functionality were assessed in 3 moments: evaluation 1 (1 week before the intervention), evaluation 2 (immediately after the last intervention), and evaluation 3 (1 week after the last intervention). The protocol consisted of 50-minute session of conventional physical therapy and visceral manipulation. The participants were randomly allocated to 2 groups: 10 for the experimental group (conventional physical therapy and visceral manipulation) and 10 for the control group (conventional physical therapy and placebo visceral manipulation).
Results: Significant reductions were found in the experimental group for lumbar mobility and specific functionality in comparison with the control group (P < .05). There were no significant differences for pain perception and global functionality.
Conclusion: The combination of visceral manipulation and conventional physical therapy program demonstrated significant between-groups differences over time for lumbar spine mobility and specific functionality. These gains occurred after 5 sessions, once a week, and were maintained 1 week after the end of the treatment. This study generated data for conduction of a power analysis to inform the design for future clinical research in this line of inquiry.
Keywords: Exercise Therapy; Low Back Pain; Manipulation, Chiropractic; Manipulation, Osteopathic; Physical Therapy Modalities; Rehabilitation; Therapy, Soft Tissue.
Figures

Similar articles
-
The effect of a six-week osteopathic visceral manipulation in patients with non-specific chronic low back pain and functional constipation: study protocol for a randomized controlled trial.Trials. 2018 Mar 2;19(1):151. doi: 10.1186/s13063-018-2532-8. Trials. 2018. PMID: 29499728 Free PMC article.
-
Immediate effects of a lumbar spine manipulation on pain sensitivity and postural control in individuals with nonspecific low back pain: a randomized controlled trial.Chiropr Man Therap. 2020 Jun 3;28(1):25. doi: 10.1186/s12998-020-00316-7. Chiropr Man Therap. 2020. PMID: 32487243 Free PMC article. Clinical Trial.
-
Complementary and alternative therapies for back pain II.Evid Rep Technol Assess (Full Rep). 2010 Oct;(194):1-764. Evid Rep Technol Assess (Full Rep). 2010. PMID: 23126534 Free PMC article. Review.
-
Short-term effectiveness of spinal manipulative therapy versus functional technique in patients with chronic nonspecific low back pain: a pragmatic randomized controlled trial.Spine J. 2016 Mar;16(3):302-12. doi: 10.1016/j.spinee.2015.08.057. Epub 2015 Sep 8. Spine J. 2016. PMID: 26362233 Clinical Trial.
-
Effectiveness of visceral fascial therapy targeting visceral dysfunctions outcome: systematic review of randomized controlled trials.BMC Complement Med Ther. 2023 Jul 31;23(1):274. doi: 10.1186/s12906-023-04099-1. BMC Complement Med Ther. 2023. PMID: 37525195 Free PMC article.
Cited by
-
On "Manual Therapy in Preadolescent Children: A Delphi Investigation of Physical Therapists in the United States." Dice JL, Dendy D, Sizer PS, Cook CE, Feuling S, Brismée JM. Phys Ther. 2021;101:pzab027. https://doi.org/10.1093/ptj/pzab027.Phys Ther. 2022 Oct 6;102(10):pzac114. doi: 10.1093/ptj/pzac114. Phys Ther. 2022. PMID: 35951675 Free PMC article. No abstract available.
-
Visceral Therapy and Physical Activity for Selected Dysfunctions, with Particular Emphasis on Locomotive Organ Pain in Pregnant Women-Importance of Reducing Oxidative Stress.Antioxidants (Basel). 2022 Jun 5;11(6):1118. doi: 10.3390/antiox11061118. Antioxidants (Basel). 2022. PMID: 35740015 Free PMC article. Review.
-
Fascial Nomenclature: Update 2021, Part 1.Cureus. 2021 Feb 14;13(2):e13339. doi: 10.7759/cureus.13339. Cureus. 2021. PMID: 33643754 Free PMC article. Review.
-
Meta-epidemiologic review: blinding and sham treatment in clinical trial design for osteopathic manipulative treatment research.Int J Osteopath Med. 2024 Mar;51:100705. doi: 10.1016/j.ijosm.2023.100705. Epub 2023 Dec 14. Int J Osteopath Med. 2024. PMID: 38312536 Free PMC article.
-
Quality of life in women with normal pregnancy.Sci Rep. 2024 May 30;14(1):12434. doi: 10.1038/s41598-024-63355-7. Sci Rep. 2024. PMID: 38816467 Free PMC article.
References
-
- Dagenais S, Caro J, Haldeman S. A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J. 2008;8(1):8–20. - PubMed
-
- Hoy D, Bain C, Williams G. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012;64(6):2028–2037. - PubMed
-
- Aluko A, DeSouza L, Peacock J. The effect of core stability exercises on variations in acceleration of trunk movement, pain, and disability during an episode of acute nonspecific low back pain: a pilot clinical trial. J Manipulative Physiol Ther. 2013;36(8):497–504.e1-3. - PubMed
-
- Bove GM, Chapelle SL. Visceral mobilization can lyse and prevent peritoneal adhesions in a rat model. J Bodyw Mov Ther. 2012;16(1):76–82. - PubMed
LinkOut - more resources
Full Text Sources
