

Changing trends in aortic valve procedures over the past ten years-from mechanical prosthesis via stented bioprosthesis to TAVI procedures-analysis of 50,846 aortic valve cases based on a Polish National Cardiac Surgery Database
- PMID: 31372271
- PMCID: PMC6626813
- DOI: 10.21037/jtd.2019.06.04
Changing trends in aortic valve procedures over the past ten years-from mechanical prosthesis via stented bioprosthesis to TAVI procedures-analysis of 50,846 aortic valve cases based on a Polish National Cardiac Surgery Database
Abstract
Background: Aortic valve replacement (AVR) is one of the most common surgeries performed in cardiac surgery operating rooms. We present actual, real life trends from the last 10 years for AVR interventions based on a multicentre National Registry of Cardiac Surgery Database.
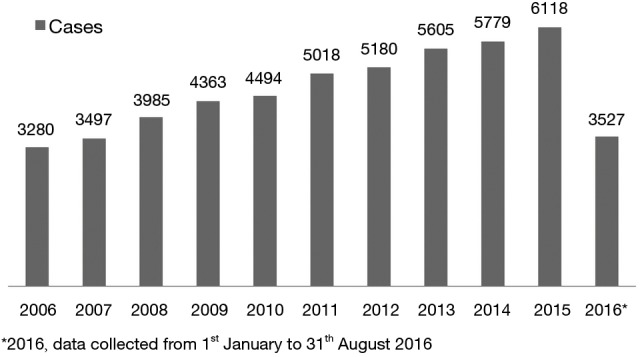
Methods: The study population consisted of all 50,846 consecutive adult patients who underwent AVR between January 2006 and August 2016 in all cardiac surgery units in Poland. The main outcome measures were changes in the number of valves, characteristics of valves, operative details, and in-hospital mortality. Analysis consisted of all aortic valve (AV) procedures, including isolated AV surgery, combination procedures and patients who had a prior valve operation.
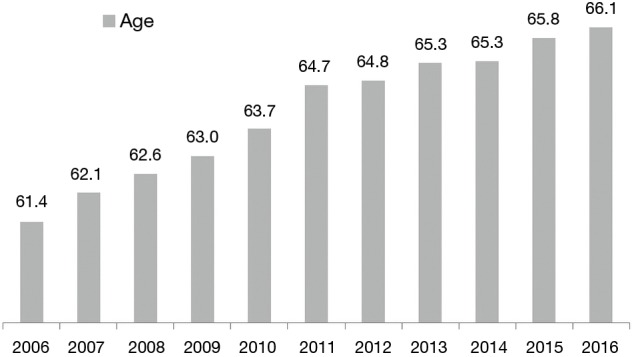
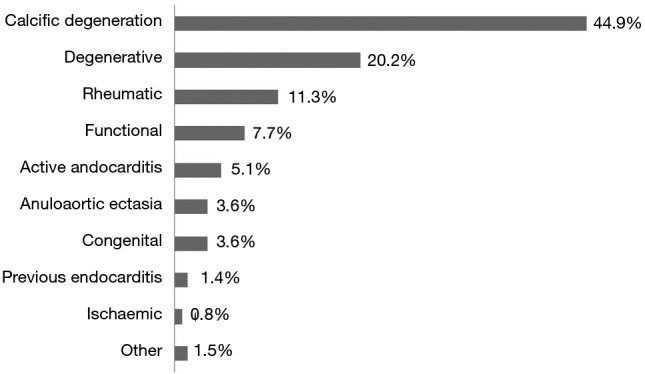
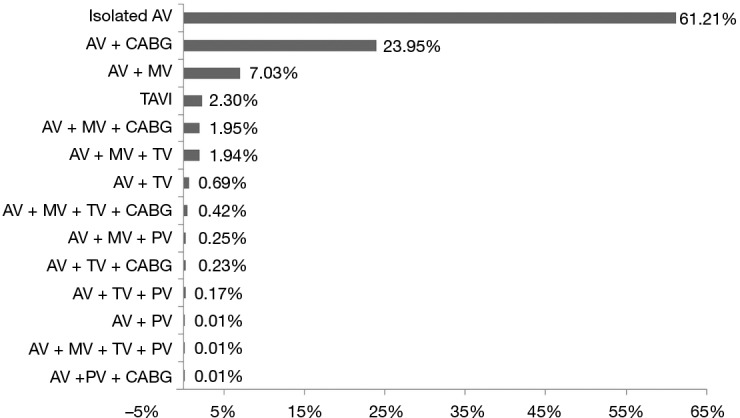
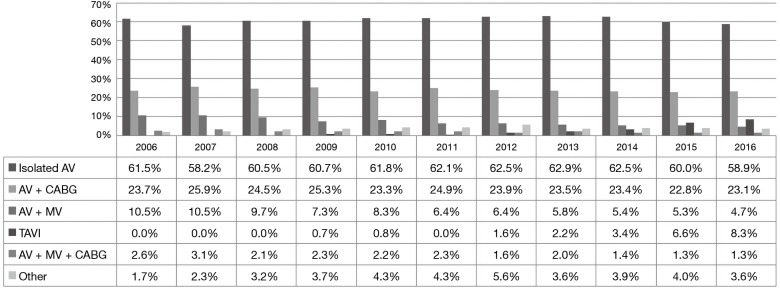
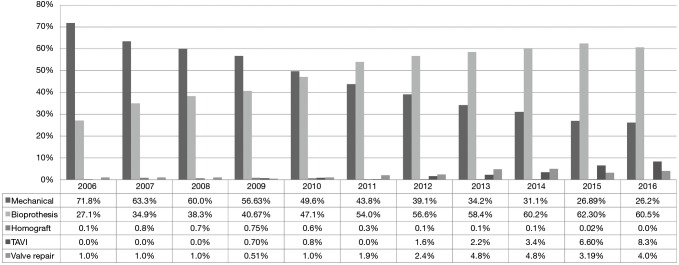
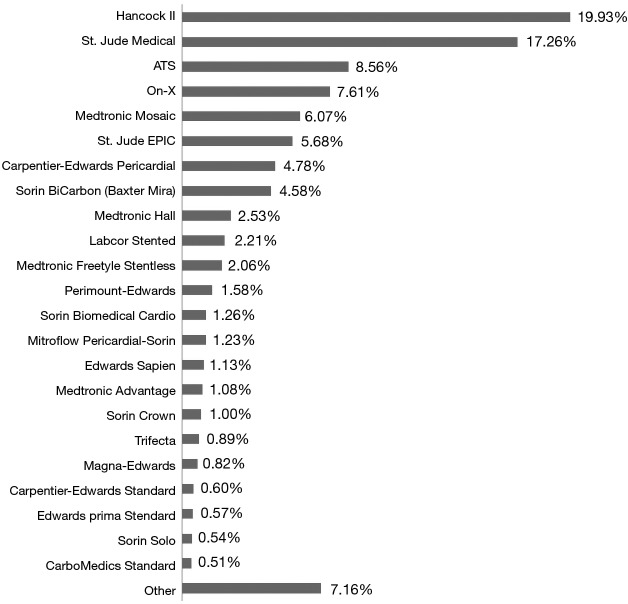
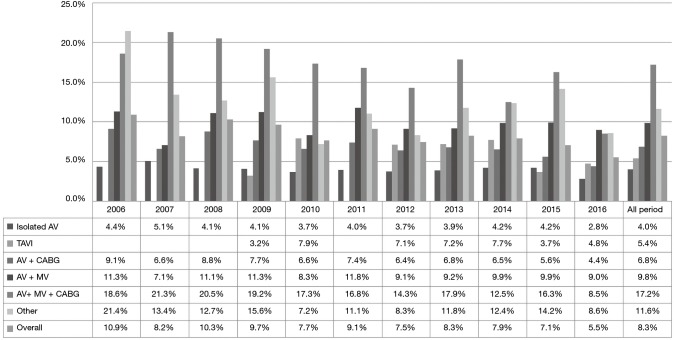
Results: In last 10 years, the number of procedures increased by 46%. Isolated surgical AVR was performed in 61.2%, AVR + coronary artery bypass grafting (CABG) in 23.9%, AVR + mitral valve replacement (MVR) in 7%, and transcatheter aortic valve implantation (TAVI) in 2.3% of patients. The mean patient age increased significantly from 61.4 years in 2006 to 66.1 years in 2016. Aortic stenosis was diagnosed in 73.4%, severe aortic insufficiency in 15.8% of cases. The most common valve pathology was calcification. Congenital valve dysfunction was diagnosed in 3.7% of cases. There was a 33.7% increase of bioprosthesis, and the most common implanted bioprosthesis was the Hancock II. The most common implanted mechanical prosthesis was the St. Jude Medical Mechanical Valve. In-hospital mortality decreased significantly over the 10-year period in all AV procedures from 10.9% in 2006 to 8.3% in 2016. Mean in-hospital mortality was: 4.0% in isolated surgical AVR, 5.4% in TAVI, 6.8% in AVR + CABG, 9.8% in AVR + MVR, 17.2% in AVR + MVR + CABG.
Conclusions: In the last ten years, the number of AV procedure has doubled. Mortality was significantly lower with all types of AV procedure despite very rapid aging of AVR patients. TAVI procedure rapidly grew in popularity. There is significant increase in the use of bioprosthesis.
Keywords: Aortic valve replacement (AVR); bioprostheses; heart valve prosthesis; mechanical prosthesis; transcatheter aortic valve implantation (TAVI).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) ., European Association for Cardio-Thoracic Surgery (EACTS)., Vahanian A, et al. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J 2012;33:2451-96. 10.1093/eurheartj/ehs109 - DOI - PubMed
-
- Brown JM, O'Brien SM, Wu C, et al. Isolated aortic valve replacement in North America comprising 108,687 patients in 10 years: changes in risks, valve types, and outcomes in the Society of Thoracic Surgeons National Database. J Thorac Cardiovasc Surg 2009;137:82-90. 10.1016/j.jtcvs.2008.08.015 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous