

Polypoid endometriosis: a mimic of malignancy
- PMID: 31372776
- PMCID: PMC8293290
- DOI: 10.1007/s00261-019-02143-8
Polypoid endometriosis: a mimic of malignancy
Abstract
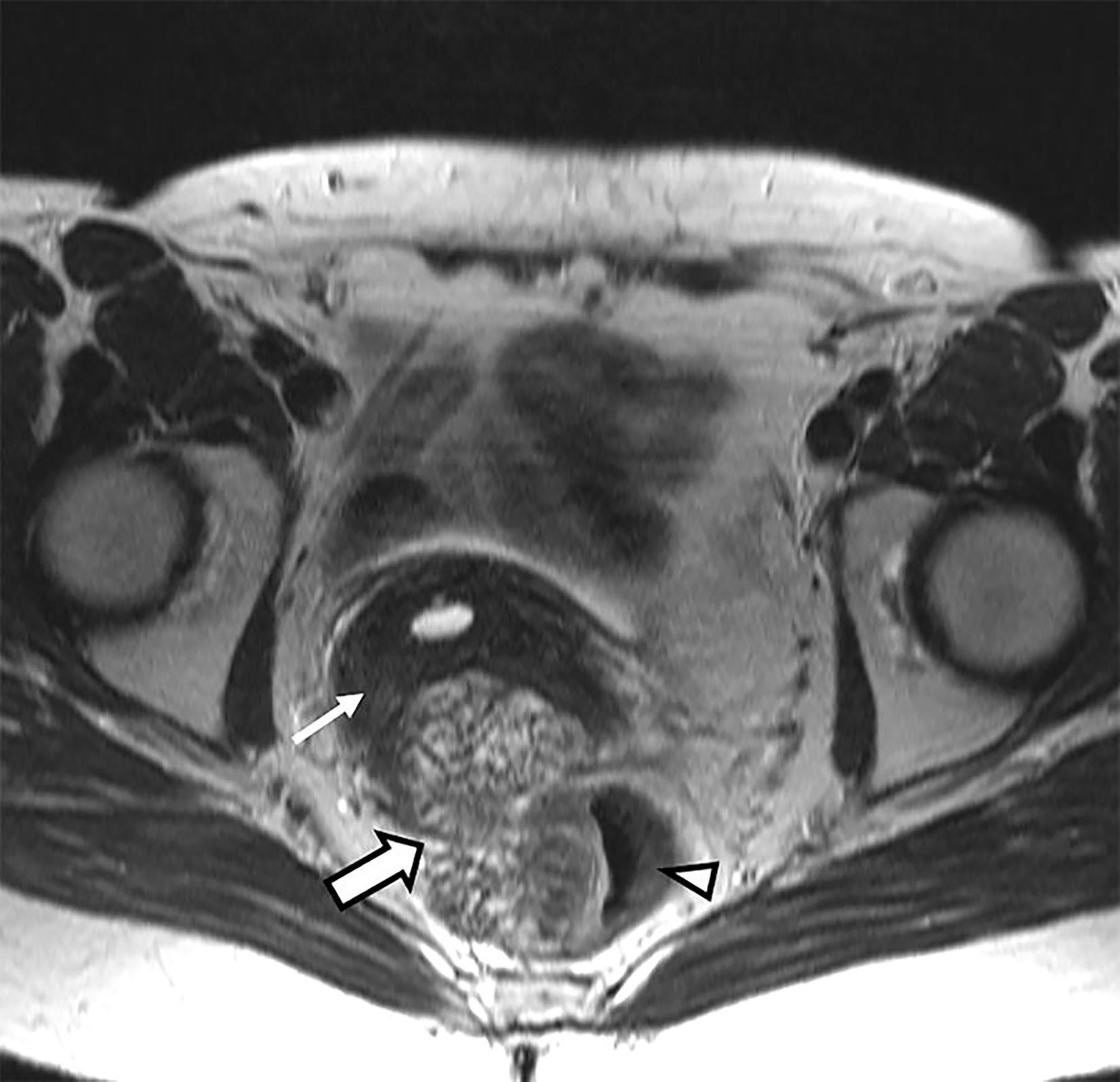
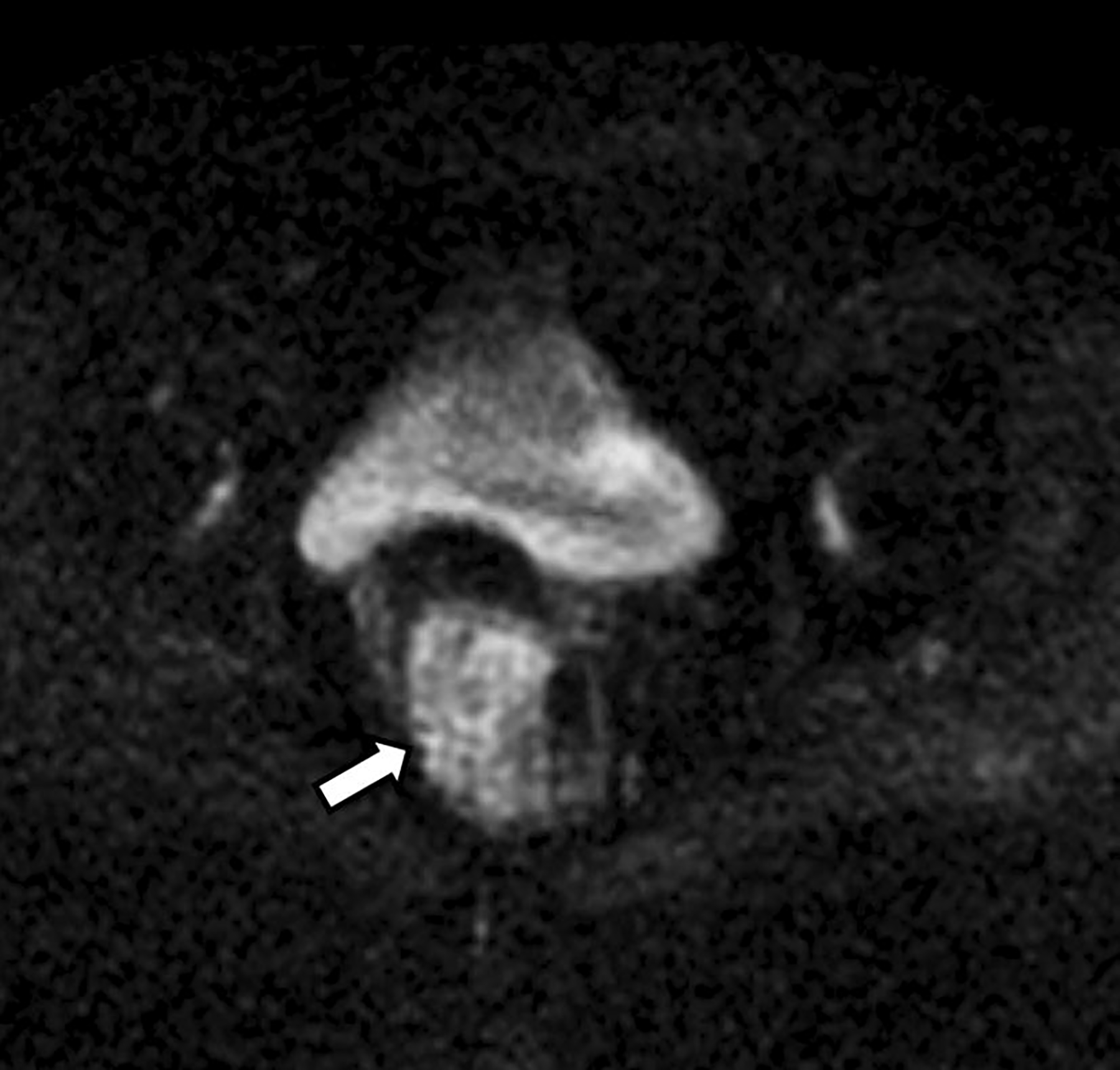
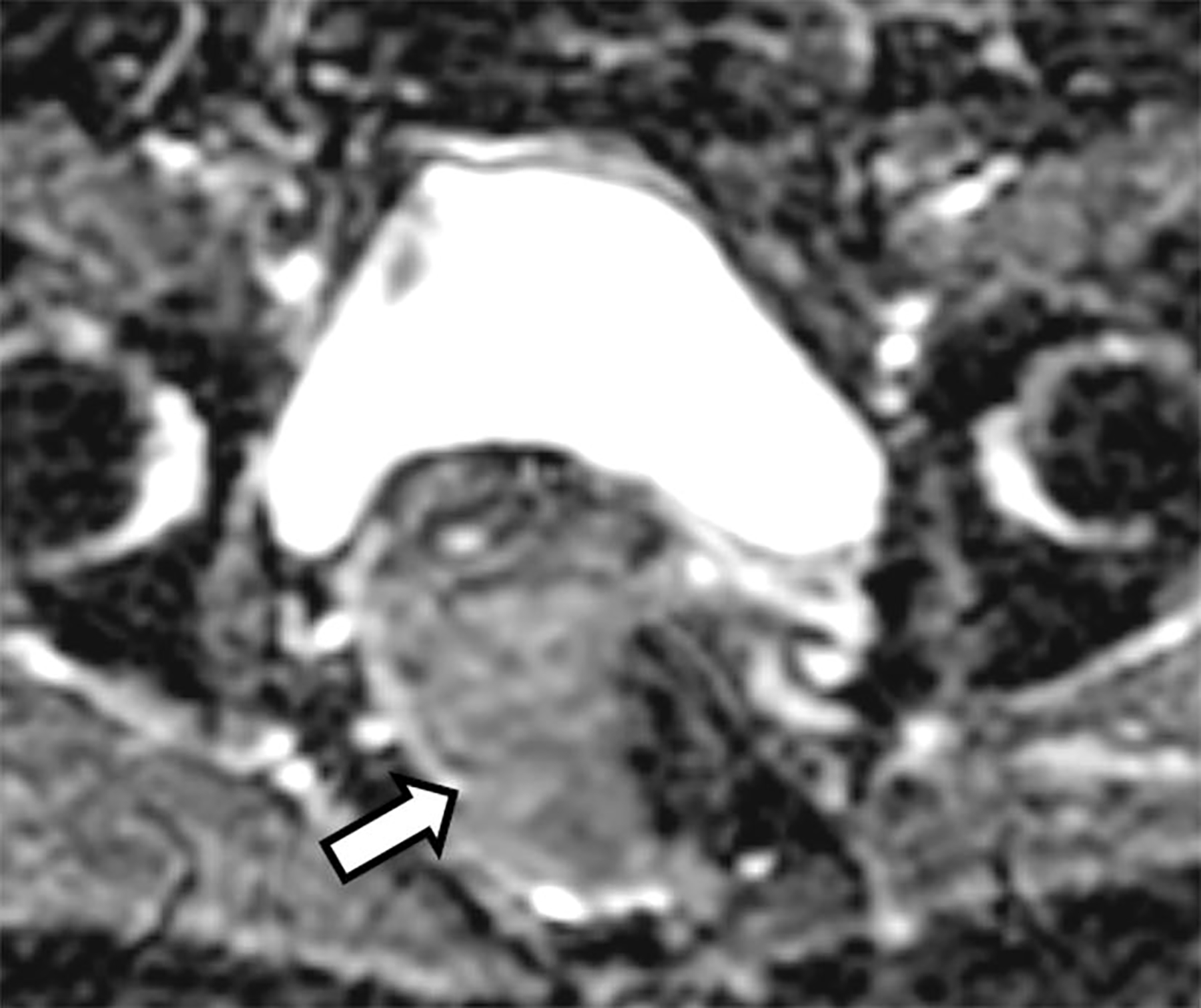
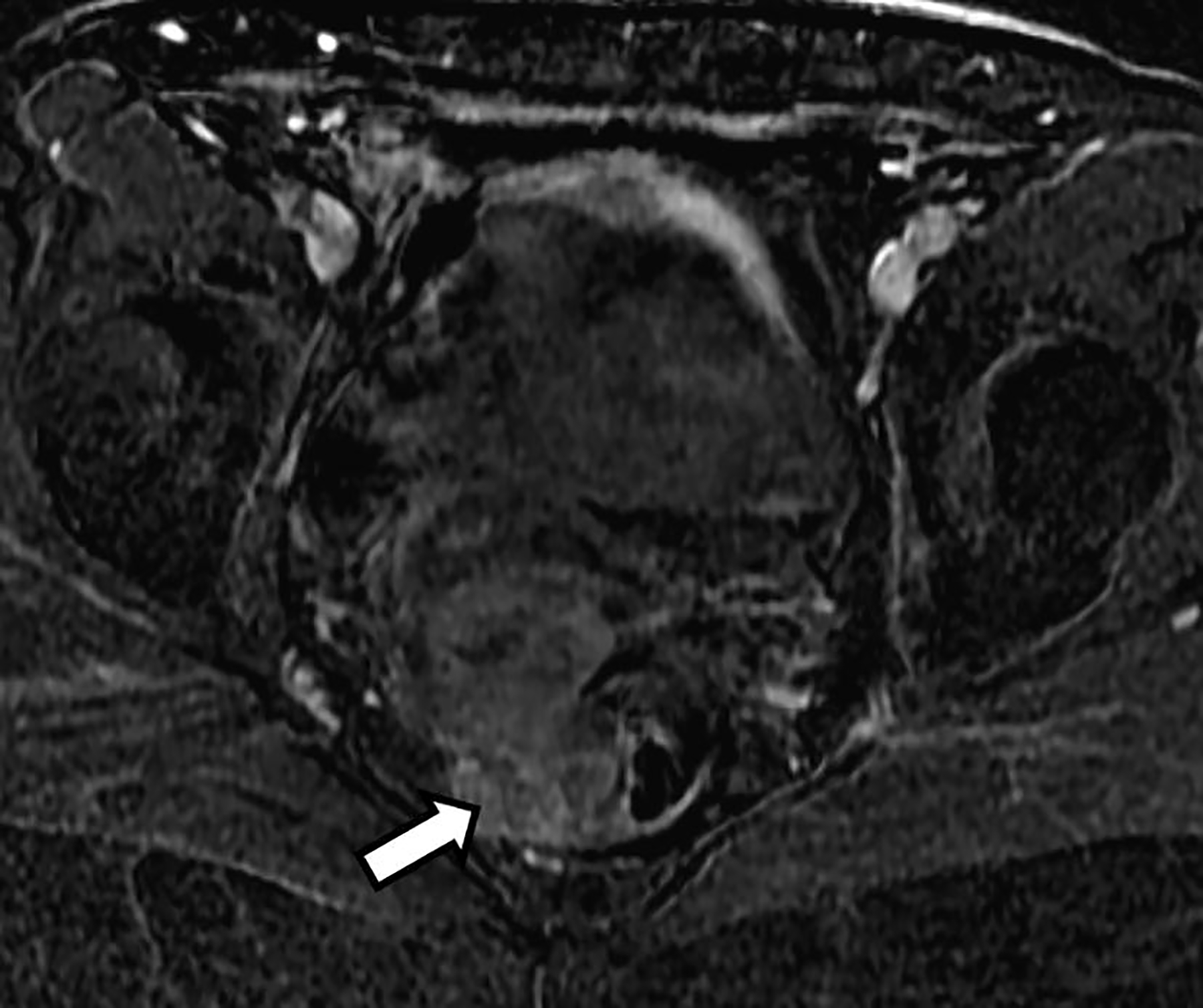
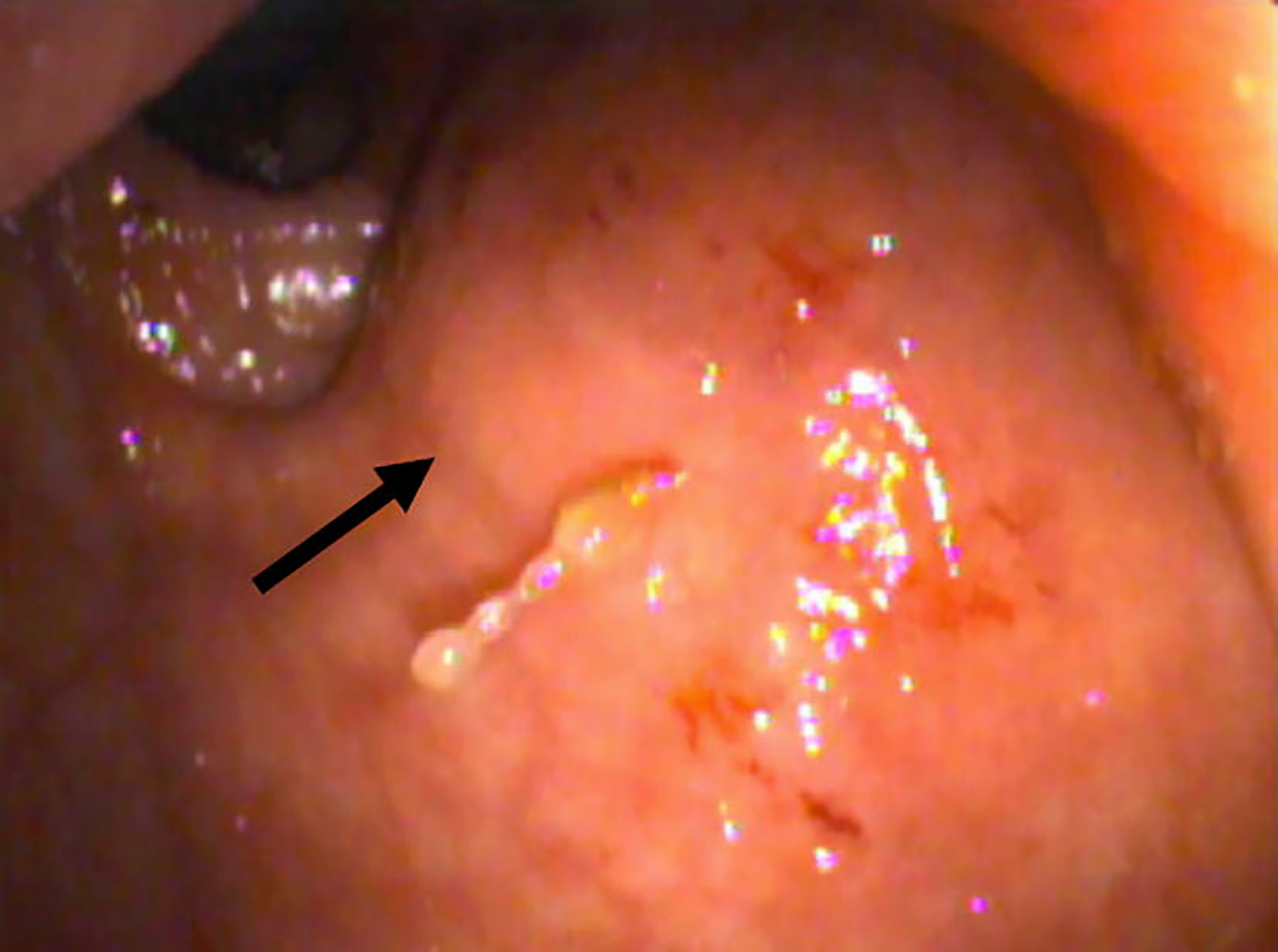
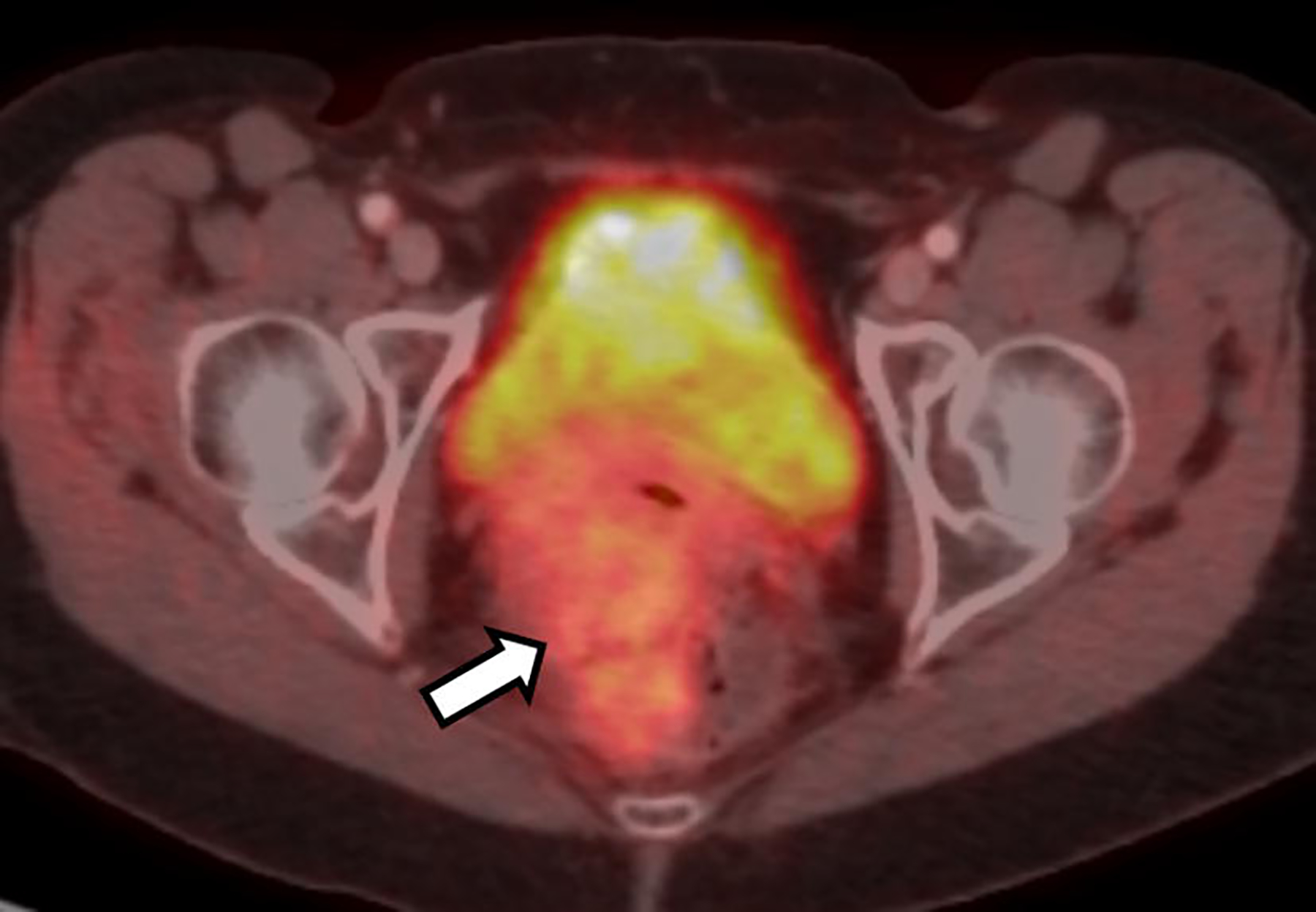
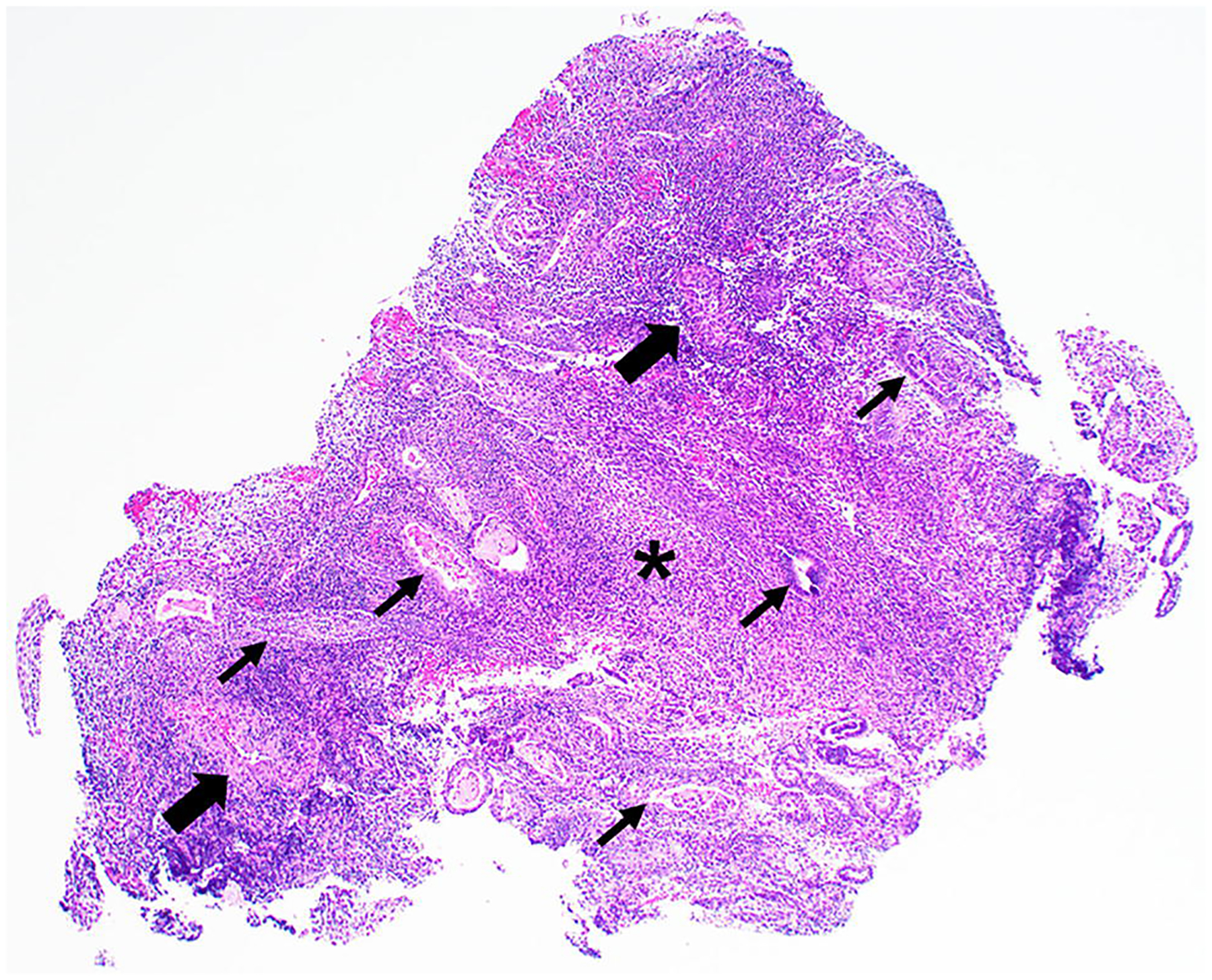
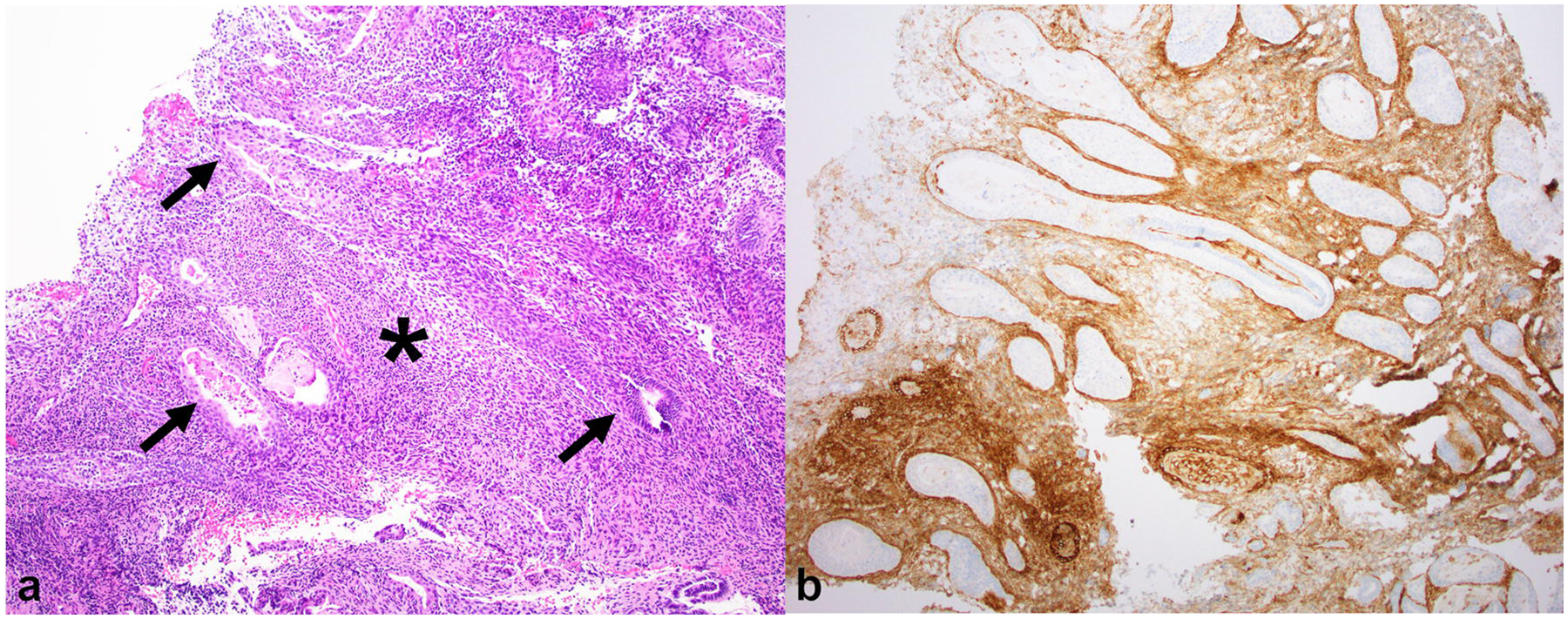
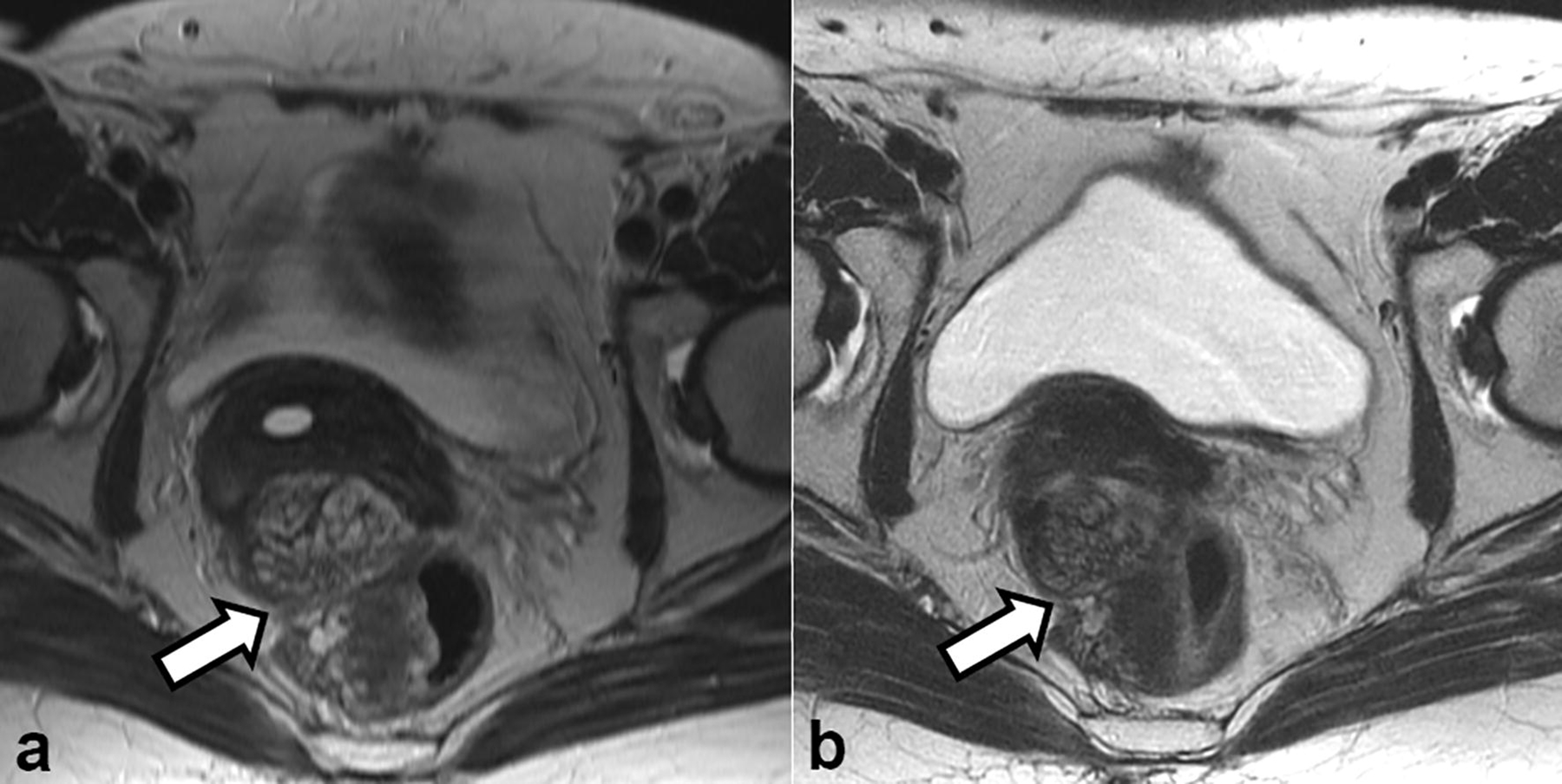
This an interesting case of an asymptomatic 60-year-old postmenopausal patient with an incidental pelvic mass mimicking a pelvic malignancy on imaging. Biopsy revealed findings consistent with polypoid endometriosis. After discontinuation of hormone replacement therapy, the mass showed decrease in size on follow-up imaging. Polypoid endometriosis is a rare but distinct variant of endometriosis with histopathologic features akin to an endometrial polyp. Clinical and imaging features of polypoid endometriosis differ from classic endometriosis. While classic endometriosis predominates in premenopausal women, polypoid endometriosis more commonly affects peri- to postmenopausal women and is associated with the exposure to Tamoxifen or hormone replacement therapy. Imaging features that aid in the diagnosis of polypoid endometriosis are a T2 hyperintense polypoid mass with signal characteristics similar to endometrium, a T2 hypointense peripheral rim, contrast enhancement pattern mirroring the enhancement of the endometrium, and lack of diffusion restriction. Radiologists should be familiar with polypoid endometriosis because this clinically and morphologically distinct variant may mimic malignant neoplasms on imaging.
Keywords: Endometriosis-associated malignancy; Magnetic resonance imaging/MRI; Polypoid endometriosis.
Conflict of interest statement
Conflicts of interest: The authors declare that they have no conflict of interest.
Figures

Similar articles
-
MR findings of polypoid endometriosis of female genital organs: report of three cases.Abdom Radiol (NY). 2022 Jun;47(6):1968-1974. doi: 10.1007/s00261-022-03530-4. Epub 2022 May 6. Abdom Radiol (NY). 2022. PMID: 35523887
-
Magnetic resonance imaging characteristics of polypoid endometriosis and review of the literature.J Obstet Gynaecol Res. 2022 Oct;48(10):2583-2593. doi: 10.1111/jog.15367. Epub 2022 Jul 22. J Obstet Gynaecol Res. 2022. PMID: 35868869 Review.
-
A case of polypoid endometriosis with malignant transformation.Abdom Radiol (NY). 2016 Sep;41(9):1699-702. doi: 10.1007/s00261-016-0696-9. Abdom Radiol (NY). 2016. PMID: 26960725
-
Polypoid endometriosis in a young female with systemic lupus erythematosus, mimicking ovarian and pelvic malignancy, a case report.Taiwan J Obstet Gynecol. 2025 Jan;64(1):166-169. doi: 10.1016/j.tjog.2024.04.022. Taiwan J Obstet Gynecol. 2025. PMID: 39794027
-
Polypoid endometriosis of the ovary mimicking ovarian carcinoma dissemination: a case report and literature review.J Obstet Gynaecol Res. 2014 May;40(5):1426-30. doi: 10.1111/jog.12358. Epub 2014 Apr 21. J Obstet Gynaecol Res. 2014. PMID: 24750503 Review.
Cited by
-
Contrast-Enhanced Ultrasound Findings of Peritoneal Polypoid Endometriosis: A Case Report and Literature Review.Int J Womens Health. 2025 May 30;17:1557-1562. doi: 10.2147/IJWH.S510066. eCollection 2025. Int J Womens Health. 2025. PMID: 40463625 Free PMC article.
-
Polypoid endometriosis of the Douglas pouch.Radiol Case Rep. 2020 Dec 30;16(3):612-614. doi: 10.1016/j.radcr.2020.12.054. eCollection 2021 Mar. Radiol Case Rep. 2020. PMID: 33456638 Free PMC article.
-
A case of polypoid endometriosis mimicking advanced ovarian carcinoma with rapid growth, invasion, and dissemination.Fukushima J Med Sci. 2022 Dec 21;68(3):183-190. doi: 10.5387/fms.2022-23. Epub 2022 Oct 27. Fukushima J Med Sci. 2022. PMID: 36288947 Free PMC article.
-
Polypoid endometriosis-An exceptional subtype of endometriosis mimicking an aggressive pelvic cancer.Clin Case Rep. 2024 Aug 28;12(9):e9343. doi: 10.1002/ccr3.9343. eCollection 2024 Sep. Clin Case Rep. 2024. PMID: 39210927 Free PMC article.
-
Mass-like extragonadal endometriosis associated malignant transformation in the pelvis: A rare case report.World J Clin Cases. 2022 Nov 6;10(31):11567-11573. doi: 10.12998/wjcc.v10.i31.11567. World J Clin Cases. 2022. PMID: 36387794 Free PMC article.
References
-
- Mostoufizadeh M, Scully RE (1980) Malignant tumors arising in endometriosis. Clinical obstetrics and gynecology 23 (3):951–963 - PubMed
-
- Parker RL, Dadmanesh F, Young RH, Clement PB (2004) Polypoid endometriosis: a clinicopathologic analysis of 24 cases and a review of the literature. The American journal of surgical pathology 28 (3):285–297 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
