

Optimal treatment for spermatogenesis in male patients with hypogonadotropic hypogonadism
- PMID: 31374027
- PMCID: PMC6709243
- DOI: 10.1097/MD.0000000000016616
Optimal treatment for spermatogenesis in male patients with hypogonadotropic hypogonadism
Abstract
Background: To compare the efficacies of gonadotropin-releasing hormone (GnRH) pulse subcutaneous infusion with combined human chorionic gonadotropin and human menopausal gonadotropin (HCG/HMG) intramuscular injection have been performed to treat male hypogonadotropic hypogonadism (HH) spermatogenesis.
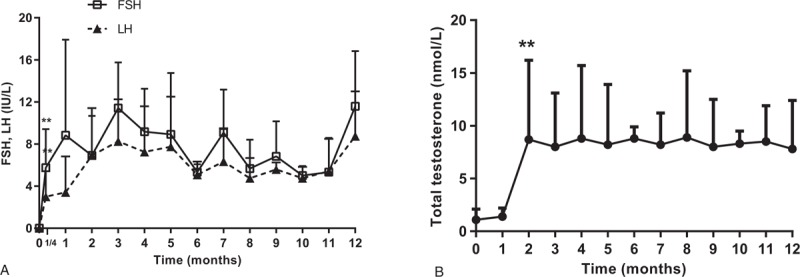
Methods: In total, 220 idiopathic/isolated HH patients were divided into the GnRH pulse therapy and HCG/HMG combined treatment groups (n = 103 and n = 117, respectively). The luteinizing hormone and follicle-stimulating hormone levels were monitored in the groups for the 1st week and monthly, as were the serum total testosterone level, testicular volume and spermatogenesis rate in monthly follow-up sessions.
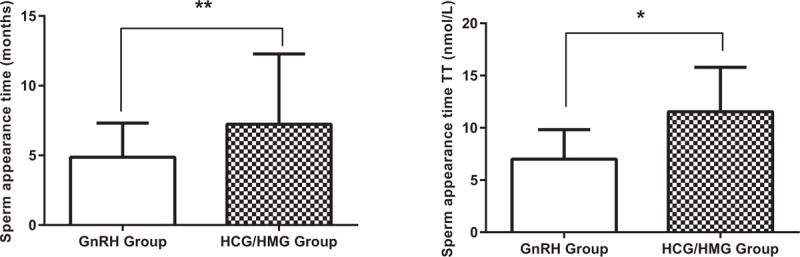
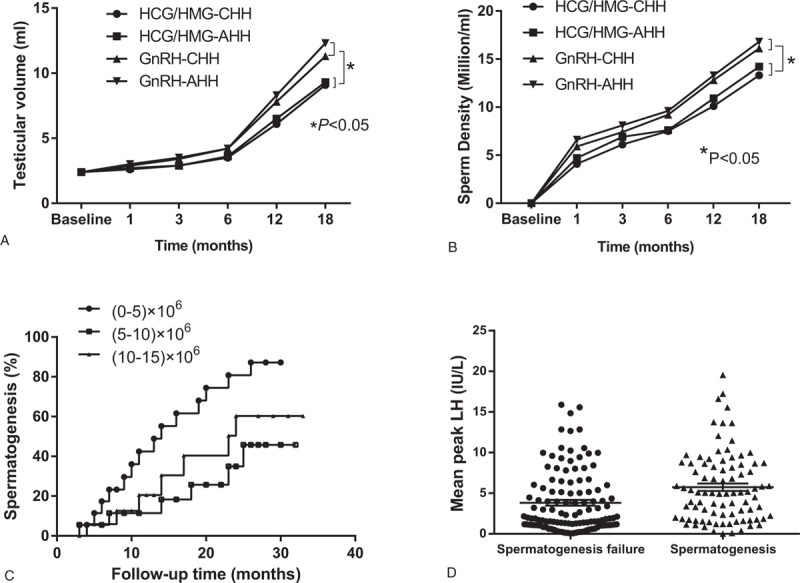
Results: In the GnRH group and HCG/HMG group, the testosterone level and testicular volume at the 6-month follow-up session were significantly higher than were those before treatment. There were 62 patients (62/117, 52.99%) in the GnRH group and 26 patients in the HCG/HMG (26/103, 25.24%) group who produced sperm following treatment. The GnRH group (6.2 ± 3.8 months) had a shorter sperm initial time than did the HCG/HMG group (10.9 ± 3.5 months). The testosterone levels in the GnRH and HCG/HMG groups were 9.8 ± 3.3 nmol/L and 14.8 ± 8.8 nmol/L, respectively.
Conclusion: The GnRH pulse subcutaneous infusion successfully treated male patients with HH, leading to earlier sperm production than that in the HCG/HMG-treated patients. GnRH pulse subcutaneous infusion is a preferred method.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Salenave S, Trabado S, Maione L, et al. Male acquired hypogonadotropic hypogonadism: diagnosis and treatment. Ann Endocrinol (Paris) 2012;73:141–6. - PubMed
-
- Varimo T, Miettinen PJ, Känsäkoski J, et al. Congenital hypogonadotropic hypogonadism, functional hypogonadotropism or constitutional delay of growth and puberty? An analysis of a large patient series from a single tertiary center. Hum Reprod 2017;32:147–53. - PubMed
-
- Sun QH, Dou JT. Diagnosis and treatment of hypogonadotropic hypogonadism in men. Drug Evaluation 2013;10:24–8.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
