

Recurrent anti-GBM disease with T-cell large granular lymphocytic leukemia: A case report
- PMID: 31374037
- PMCID: PMC6708844
- DOI: 10.1097/MD.0000000000016649
Recurrent anti-GBM disease with T-cell large granular lymphocytic leukemia: A case report
Abstract
Rationale: Anti-glomerular basement membrane disease (anti-GBM disease) is a rare small vessel vasculitis caused by autoantibodies directed against the glomerular and alveolar basement membranes. Anti-GBM disease is usually a monophasic illness and relapse is rare after effective treatment. This article reports a case of coexistence of recurrent anti-GBM disease and T-cell large granular lymphocytic (T-LGL) leukemia.
Patient concerns: A 37-year-old man presented with hematuria, edema, and acute kidney injury for 2 months.
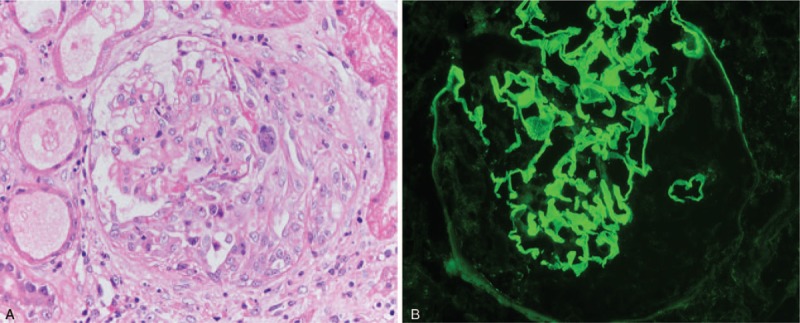
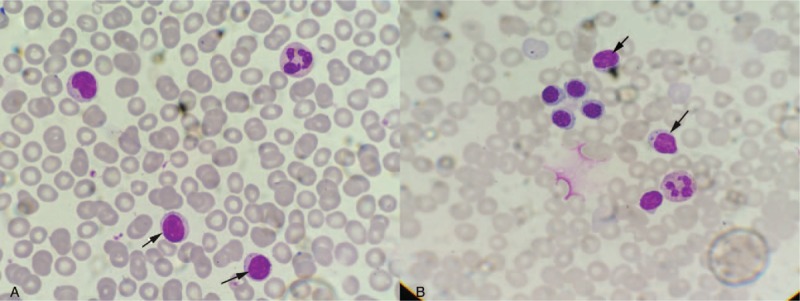
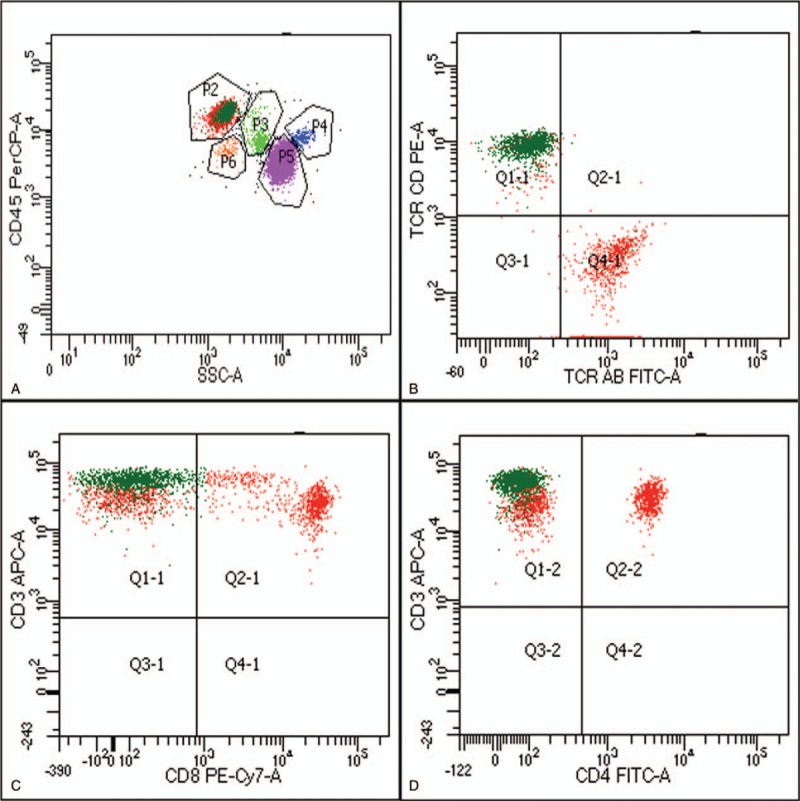
Diagnosis: Anti-GBM disease was diagnosed by renal biopsy, in which crescentic glomerulonephritis was observed with light microscopy, strong linear immunofluorescent staining for immunoglobulin G on the GBM and positive serum anti-GBM antibody. Given this diagnosis, the patient was treated with plasmapheresis, steroids, and cyclophosphamide for 4 months. The anti-GBM antibody titer was maintained to negative level but the patient remained dialysis-dependent. One year later, the patient suffered with a relapse of anti-GBM disease, after an extensive examination, he was further diagnosed T-LGL leukemia by accident.
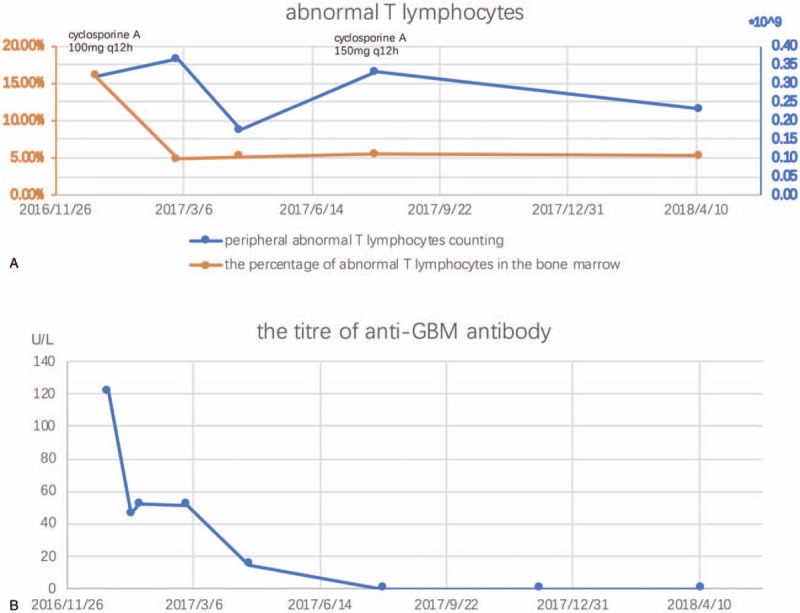
Interventions: The patient received cyclosporine A therapy for T-LGL leukemia.
Outcomes: After treatment with cyclosporine A, serum anti-GBM antibody became undetectable. During the 16 months follow-up, anti-GBM titer remained normal and abnormal T-lymphocytes in the bone marrow and peripheral blood were also decreased.
Lessons: T-LGL leukemia is an indolent lymphoproliferative disorder that represents a monoclonal expansion of cytotoxic T cells, which has been reported to be accompanied by some autoimmune diseases. This is the first report of coincidence of T-LGL leukemia and anti-GBM disease, and suggests there are some relationships between these 2 diseases. Clinical physicians should exclude hematological tumors when faced with recurrent anti-GBM disease.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Saus J, Wieslander J, Langeveld JP, et al. Identification of the Goodpasture antigen as the alpha 3 (IV) chain of collagen IV. J Biol Chem 1988;263:13374–80. - PubMed
-
- Levy JB, Turner AN, Rees AJ, et al. Long-term outcome of anti-glomerular basement membrane antibody disease treated with plasma exchange and immunosuppression. Ann Intern Med 2001;134:1033–42. - PubMed
-
- Audemard A, Lamy T, Bareau B, et al. Vasculitis associated with large granular lymphocyte (LGL) leukemia: presentation and treatment outcomes of 11 cases. Semin Arthritis Rheum 2013;43:362–6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
