

The neuropathological diagnosis of Alzheimer's disease
- PMID: 31375134
- PMCID: PMC6679484
- DOI: 10.1186/s13024-019-0333-5
The neuropathological diagnosis of Alzheimer's disease
Abstract
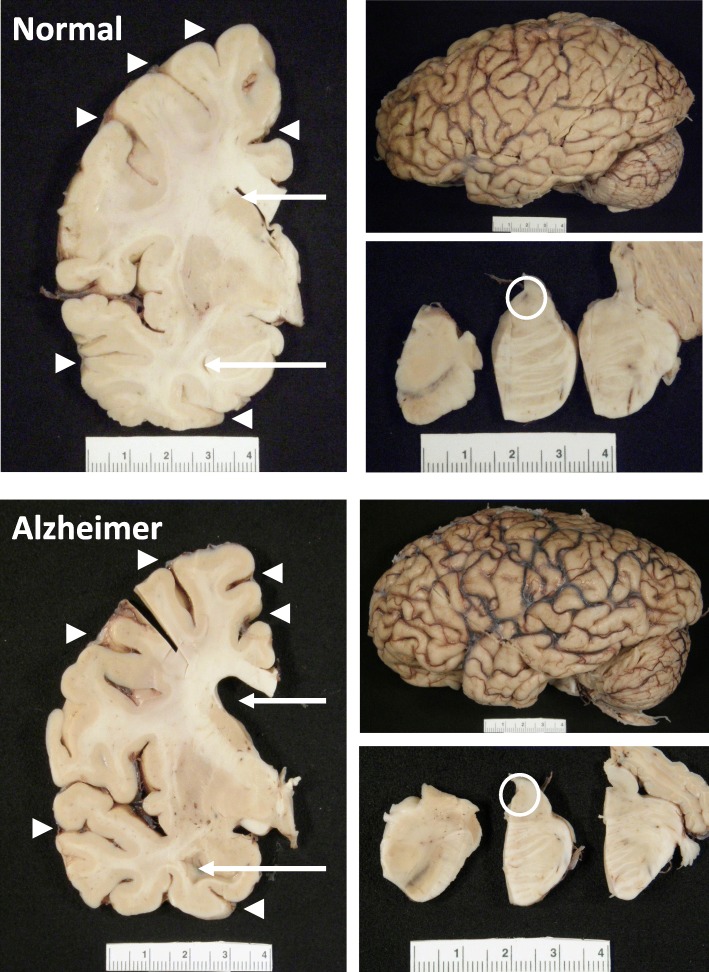
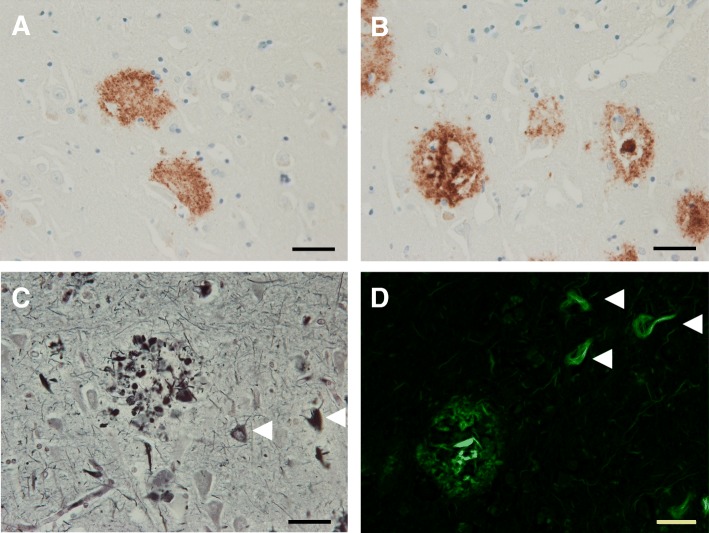
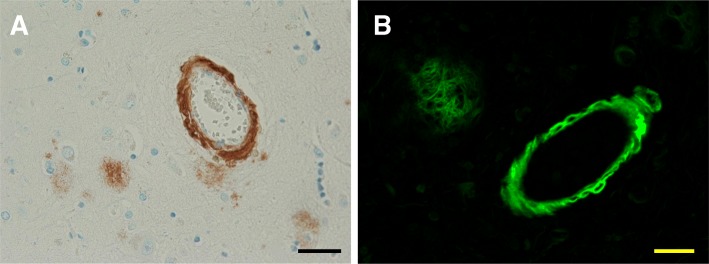
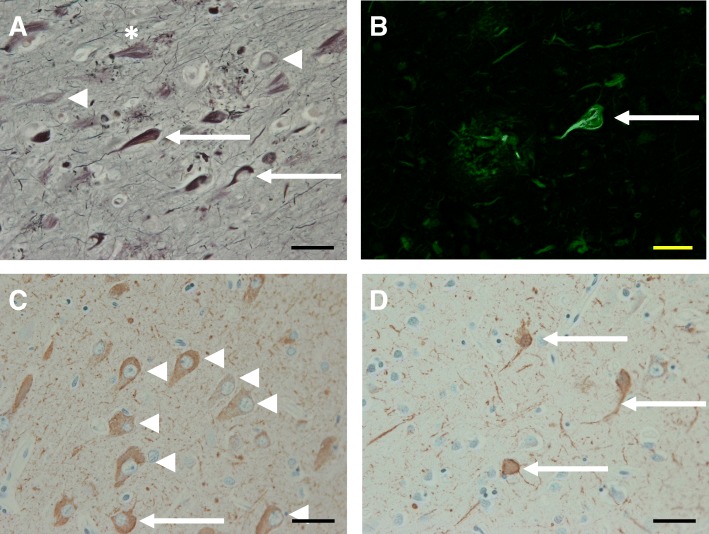
Alzheimer's disease is a progressive neurodegenerative disease most often associated with memory deficits and cognitive decline, although less common clinical presentations are increasingly recognized. The cardinal pathological features of the disease have been known for more than one hundred years, and today the presence of these amyloid plaques and neurofibrillary tangles are still required for a pathological diagnosis. Alzheimer's disease is the most common cause of dementia globally. There remain no effective treatment options for the great majority of patients, and the primary causes of the disease are unknown except in a small number of familial cases driven by genetic mutations. Confounding efforts to develop effective diagnostic tools and disease-modifying therapies is the realization that Alzheimer's disease is a mixed proteinopathy (amyloid and tau) frequently associated with other age-related processes such as cerebrovascular disease and Lewy body disease. Defining the relationships between and interdependence of various co-pathologies remains an active area of investigation. This review outlines etiologically-linked pathologic features of Alzheimer's disease, as well as those that are inevitable findings of uncertain significance, such as granulovacuolar degeneration and Hirano bodies. Other disease processes that are frequent, but not inevitable, are also discussed, including pathologic processes that can clinically mimic Alzheimer's disease. These include cerebrovascular disease, Lewy body disease, TDP-43 proteinopathies and argyrophilic grain disease. The purpose of this review is to provide an overview of Alzheimer's disease pathology, its defining pathologic substrates and the related pathologies that can affect diagnosis and treatment.
Keywords: Alzheimer’s disease; Amyloid plaques; Neurofibrillary tangles; Neuropathology.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Schultz C., Del Tredici K.H.B: Neuropathology of Alzheimer’s Disease. In Alzheimer’s Disease Current Clinical Neurology. Edited by R. R, B. R. Totowa, NJ: Humana Press; 2004.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
