

18F-fluciclovine PET-CT and 68Ga-PSMA-11 PET-CT in patients with early biochemical recurrence after prostatectomy: a prospective, single-centre, single-arm, comparative imaging trial
- PMID: 31375469
- PMCID: PMC7469487
- DOI: 10.1016/S1470-2045(19)30415-2
18F-fluciclovine PET-CT and 68Ga-PSMA-11 PET-CT in patients with early biochemical recurrence after prostatectomy: a prospective, single-centre, single-arm, comparative imaging trial
Erratum in
-
Correction to Lancet Oncol 2019; 20: 1286-94.Lancet Oncol. 2019 Nov;20(11):e613. doi: 10.1016/S1470-2045(19)30593-5. Epub 2019 Sep 23. Lancet Oncol. 2019. PMID: 31558425 No abstract available.
-
Correction to Lancet Oncol 2019; 20: 1286-94.Lancet Oncol. 2020 Jun;21(6):e304. doi: 10.1016/S1470-2045(20)30279-5. Lancet Oncol. 2020. PMID: 32502456 No abstract available.
Abstract
Background: National Comprehensive Cancer Network guidelines consider 18F-fluciclovine PET-CT for prostate cancer biochemical recurrence localisation after radical prostatectomy, whereas European Association of Urology guidelines recommend prostate-specific membrane antigen (PSMA) PET-CT. To the best of our knowledge, no prospective head-to-head comparison between these tests has been done so far. The aim of this study was to compare prospectively paired 18F-fluciclovine and PSMA PET-CT scans for localising biochemical recurrence of prostate cancer after radical prostatectomy in patients with low prostate-specific antigen (PSA) concentrations (<2·0 ng/mL).
Methods: This was a prospective, single-centre, open-label, single-arm comparative study done at University of California Los Angeles (Los Angeles, CA, USA). Patients older than 18 years of age with prostate cancer biochemical recurrence after radical prostatectomy and PSA levels ranging from 0·2 to 2·0 ng/mL without any prior salvage therapy and with a Karnofsky performance status of at least 50 were eligible. Patients underwent 18F-fluciclovine (reference test) and PSMA (index test) PET-CT scans within 15 days. Detection rate of biochemical recurrence at the patient level and by anatomical region was the primary endpoint. A statistical power analysis demonstrated that a sample size of 50 patients was needed to show a 22% difference in detection rates in favour of PSMA (test for superiority). Each PET scan was interpreted by three independent masked readers and a consensus majority interpretation was generated (two vs one) to determine positive findings. This study is registered with ClinicalTrials.gov, number NCT02940262, and is complete.
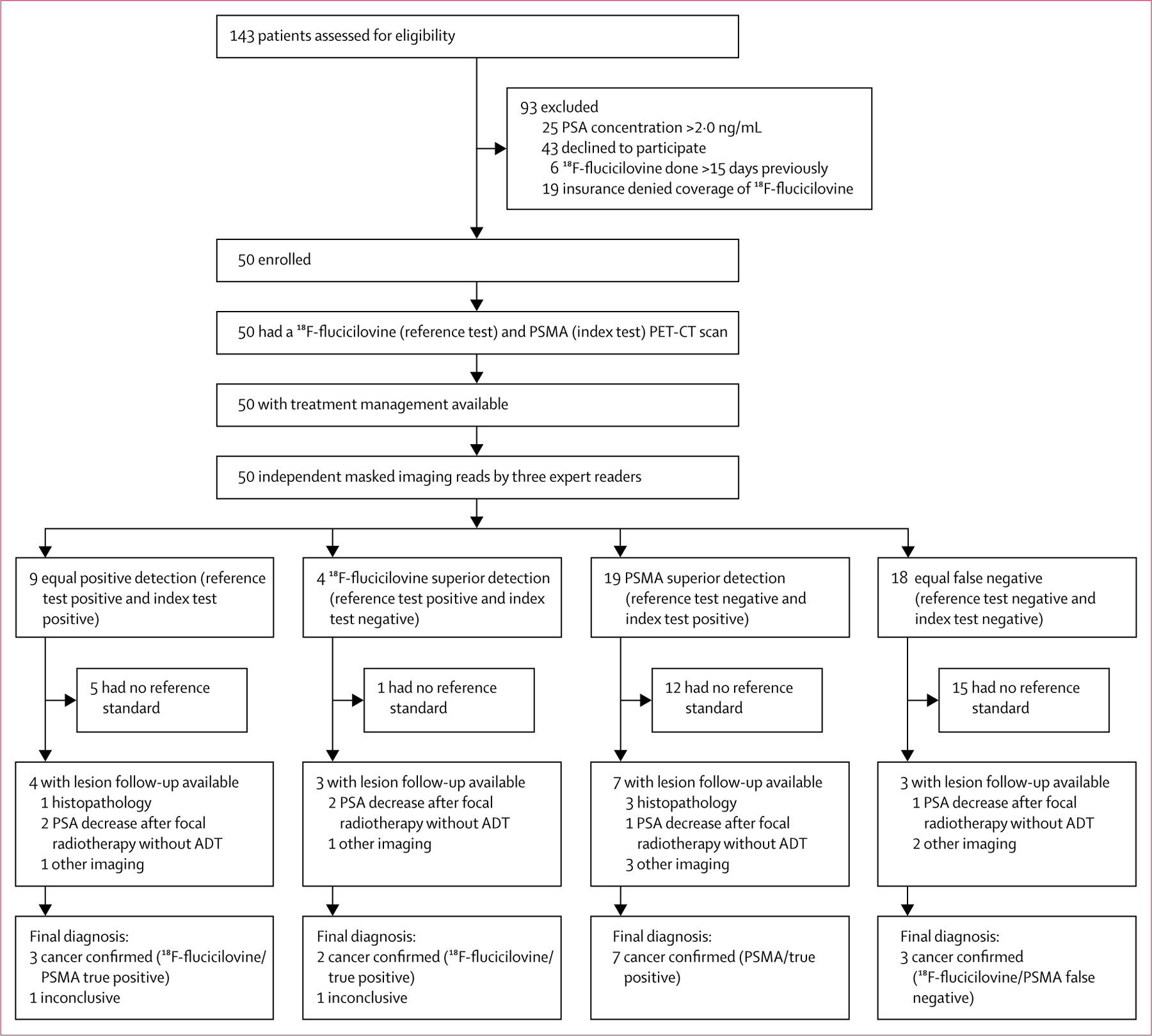
Findings: Between Feb 26, 2018, and Sept 20, 2018, 143 patients were screened for eligibility, of whom 50 patients were enrolled into the study. Median follow-up was 8 months (IQR 7-9). The primary endpoint was met; detection rates were significantly lower with 18F-fluciclovine PET-CT (13 [26%; 95% CI 15-40] of 50) than with PSMA PET-CT (28 [56%; 41-70] of 50), with an odds ratio (OR) of 4·8 (95% CI 1·6-19·2; p=0·0026) at the patient level; in the subanalysis of the pelvic nodes region (four [8%; 2-19] with 18F-fluciclovine vs 15 [30%; 18-45] with PSMA PET-CT; OR 12·0 [1·8-513·0], p=0·0034); and in the subanalysis of any extrapelvic lesions (none [0%; 0-6] vs eight [16%; 7-29]; OR non-estimable [95% CI non-estimable], p=0·0078).
Interpretation: With higher detection rates, PSMA should be the PET tracer of choice when PET-CT imaging is considered for subsequent treatment management decisions in patients with prostate cancer and biochemical recurrence after radical prostatectomy and low PSA concentrations (≤2·0 ng/mL). Further research is needed to investigate whether higher detection rates translate into improved oncological outcomes.
Funding: None.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests
JCa reports personal fees from Progenics Pharmaceuticals and RadioMedix and is a consultant for Blue Earth Diagnostics outside the submitted work. JCz is a founder, board member, and holds equity in Sofie Biosciences and Trethera Therapeutics, serves on the medical advisory board of Actinium, and is a member of the VISION trial steering committee, a clinical trial sponsored by Endocyte, outside the submitted work. WPF is a consultant for Endocyte and Ipsen and reports personal fees from Radiomedix Inc outside the submitted work. ME reports grants from ABX advanced biochemical compounds and Blue Earth Diagnostics, is a consultant for Progenics Pharmaceuticals and Janssen, and has a patent rhPSMA issued, outside the submitted work. TB-G reports grants and personal fees from Blue Earth Diagnostics outside the submitted work. BS-B reports grants and personal fees from Blue Earth Diagnostics and personal fees from Phillips outside the submitted work. CN reports grants and personal fees from Blue Earth Diagnostics outside the submitted work. TAH reports grants from Advanced Accelerator Applications and personal fees from GE Healthcare, Progenics Pharmaceuticals, Curium, and Ipsen outside the submitted work. MBR reports grants and non-financial support from Novartis, personal fees and non-financial support from Johnson & Johnson, non-financial support from Merck, Medivation, and Astellas, and has a patent “Inhibitors of the N-terminal Domain of the Androgen Receptor” pending, outside the submitted work. MSH reports grants and personal fees from Endocyte, Ipsen, and Sanofi Genzyme outside the submitted work. CR received speaker fees from GE Healthcare outside the submitted work. AUK reports personal fees from Varian Medical Systems, ViewRay, and Janssen Pharmaceuticals outside the submitted work. HJ is an investigator for ImaginAb and Subtle Medical outside the submitted work. All other authors declare no competing interests.
Figures

Comment in
-
The emerging role of PET-CT scan after radical prostatectomy: still a long way to go.Lancet Oncol. 2019 Sep;20(9):1193-1195. doi: 10.1016/S1470-2045(19)30501-7. Epub 2019 Jul 30. Lancet Oncol. 2019. PMID: 31375470 No abstract available.
-
What is the best PET target for early biochemical recurrence of prostate cancer?Lancet Oncol. 2019 Nov;20(11):e608. doi: 10.1016/S1470-2045(19)30586-8. Lancet Oncol. 2019. PMID: 31674313 No abstract available.
-
What is the best PET target for early biochemical recurrence of prostate cancer?-Authors' reply.Lancet Oncol. 2019 Nov;20(11):e609-e610. doi: 10.1016/S1470-2045(19)30654-0. Lancet Oncol. 2019. PMID: 31674314 No abstract available.
-
Re: 18F-Fluciclovine PET-CT and 68Ga-PSMA-11 PET-CT in Patients with Early Biochemical Recurrence After Prostatectomy: A Prospective, Single-centre, Single-arm, Comparative Imaging Trial.Eur Urol. 2020 Mar;77(3):392-393. doi: 10.1016/j.eururo.2019.10.018. Epub 2019 Nov 20. Eur Urol. 2020. PMID: 31759768 No abstract available.
-
Re: 18F-Fluciclovine PET-CT and 68Ga-PSMA-11 PET-CT in Patients with Early Biochemical Recurrence after Prostatectomy: A Prospective, Single-Centre, Single-Arm, Comparative Imaging Trial.J Urol. 2020 Apr;203(4):661-662. doi: 10.1097/JU.0000000000000730. Epub 2020 Jan 13. J Urol. 2020. PMID: 31928460 No abstract available.
-
New metabolic tracers for detectable PSA levels in the post-prostatectomy setting: is the era of melting glaciers upcoming?Transl Androl Urol. 2019 Dec;8(Suppl 5):S538-S541. doi: 10.21037/tau.2019.12.34. Transl Androl Urol. 2019. PMID: 32042641 Free PMC article. No abstract available.
-
Commentary RE: Upregulation of PSMA Following Androgen Deprivation Therapy.Urology. 2020 Nov;145:329-330. doi: 10.1016/j.urology.2020.04.027. Epub 2020 Apr 15. Urology. 2020. PMID: 32304680 No abstract available.
References
-
- National Comprehensive Cancer Network. Guidelines for treatment of cancer by site: prostate cancer. Version 4 2018. https://www.nccn.org/professionals/physician_gls/default.aspx#prostate (accessed March 13, 2019).
-
- European Association of Urology. Prostate cancer 2018. Uroweb. https://uroweb.org/guideline/prostate-cancer/ (accessed March 13, 2019 ).
-
- Nanni C, Zanoni L, Pultrone C, et al. (18)F-FACBC (anti1-amino-3-(18)F-fluorocyclobutane-1-carboxylic acid) versus (11)C-choline PET/CT in prostate cancer relapse: results of a prospective trial. Eur J Nucl Med Mol Imaging 2016; 43: 1601–10. - PubMed
-
- Morigi JJ, Stricker PD, van Leeuwen PJ, et al. Prospective comparison of 18F-fluoromethylcholine versus 68Ga-PSMA PET/CT in prostate cancer patients who have rising PSA after curative treatment and are being considered for targeted therapy. J Nucl Med 2015; 56: 1185–90. - PubMed
-
- Calais J, Fendler WP, Herrmann K, Eiber M, Ceci F. Comparison of 68Ga-PSMA-11 and 18F-fluciclovine PET/CT in a case series of 10 patients with prostate cancer recurrence. J Nucl Med 2018; 59: 789–94. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
