

Chronic Granulomatous Disease-Associated IBD Resolves and Does Not Adversely Impact Survival Following Allogeneic HCT
- PMID: 31376032
- PMCID: PMC6754755
- DOI: 10.1007/s10875-019-00659-8
Chronic Granulomatous Disease-Associated IBD Resolves and Does Not Adversely Impact Survival Following Allogeneic HCT
Erratum in
-
Correction: Chronic Granulomatous Disease-Associated IBD Resolves and Does Not Adversely Impact Survival Following Allogeneic HCT.J Clin Immunol. 2020 Nov;40(8):1211-1213. doi: 10.1007/s10875-020-00852-0. J Clin Immunol. 2020. PMID: 32860171 Free PMC article.
Abstract
Introduction: Inflammatory bowel disease (IBD) affects approximately 1/3 of patients with chronic granulomatous disease (CGD). Comprehensive investigation of the effect of allogeneic hematopoietic cell transplantation (HCT) on CGD IBD and the impact of IBD on transplant outcomes is lacking.
Methods: We collected data retrospectively from 145 patients with CGD who had received allogeneic HCT at 26 Primary Immune Deficiency Treatment Consortium (PIDTC) centers between January 1, 2005 and June 30, 2016.
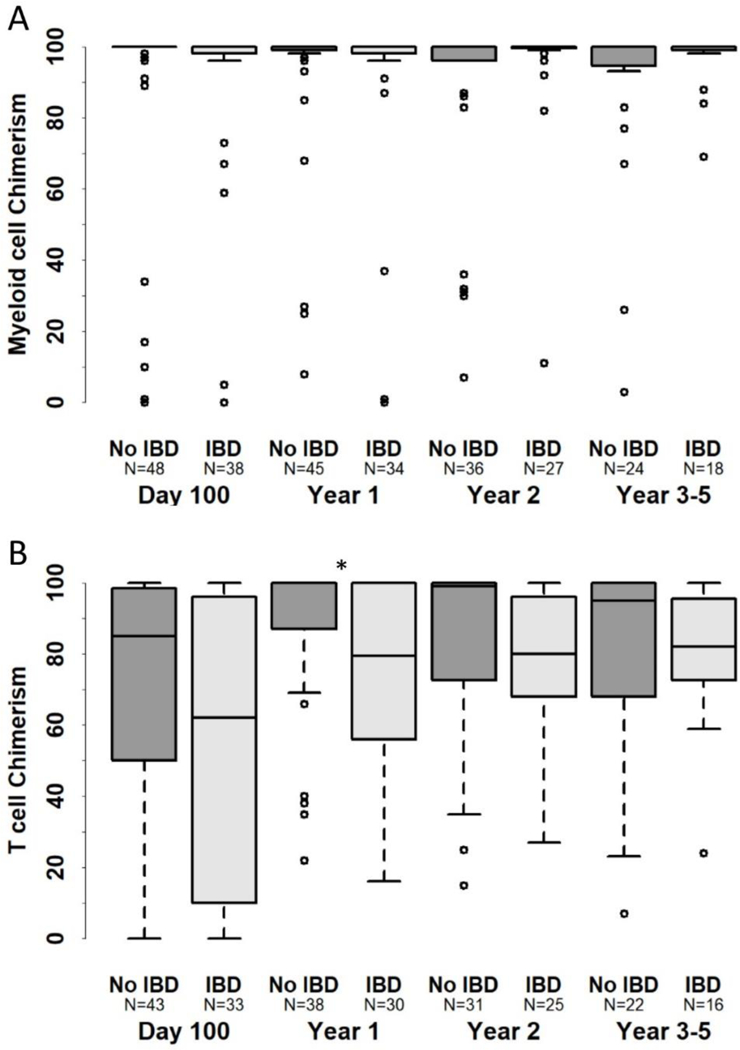
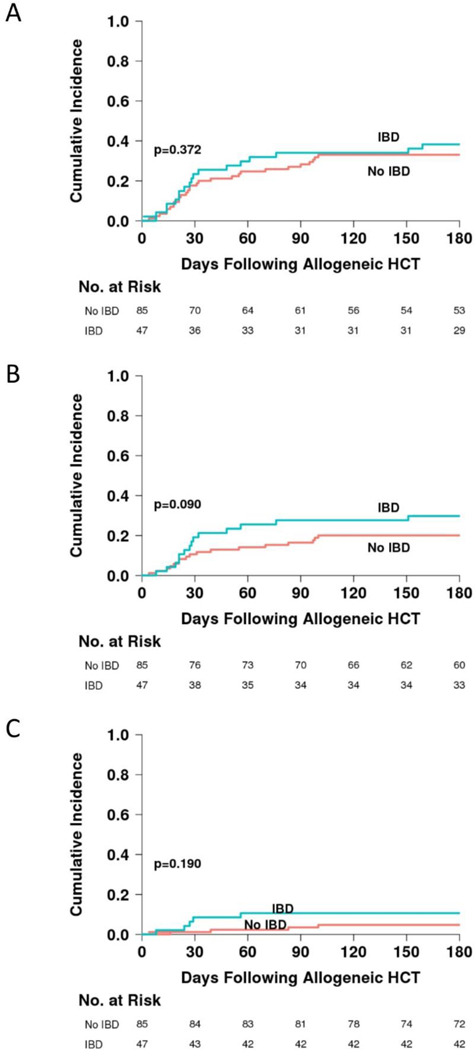
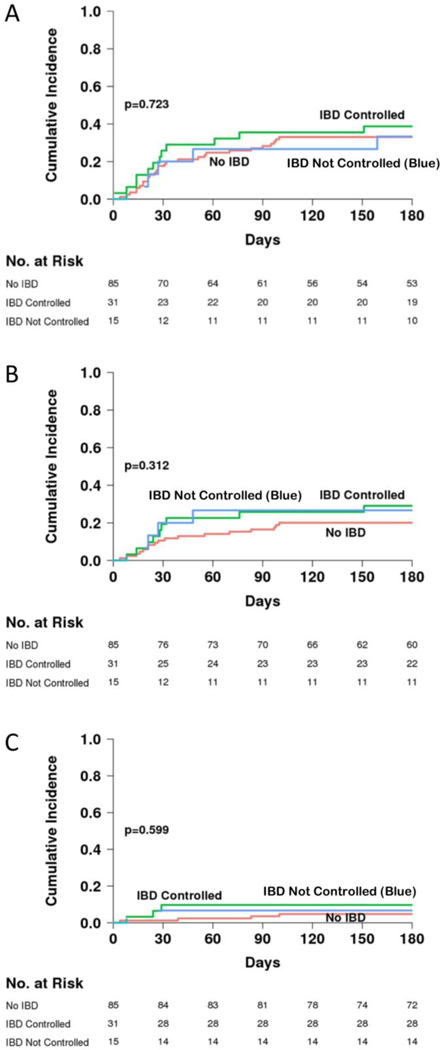
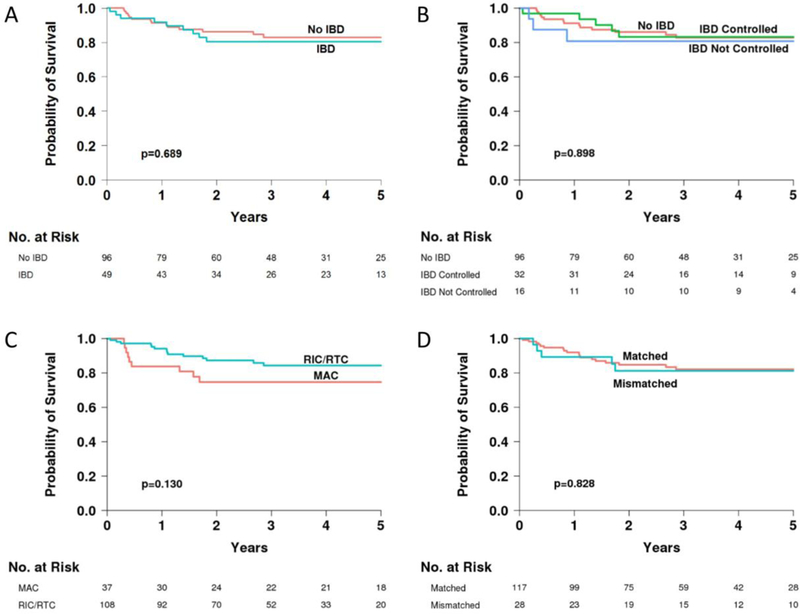
Results: Forty-nine CGD patients with IBD and 96 patients without IBD underwent allogeneic HCT. Eighty-nine percent of patients with IBD and 93% of patients without IBD engrafted (p = 0.476). Upper gastrointestinal acute GVHD occurred in 8.5% of patients with IBD and 3.5% of patients without IBD (p = 0.246). Lower gastrointestinal acute GVHD occurred in 10.6% of patients with IBD and 11.8% of patients without IBD (p = 0.845). The cumulative incidence of acute GVHD grades II-IV was 30% (CI 17-43%) in patients with IBD and 20% (CI 12-29%) in patients without IBD (p = 0.09). Five-year overall survival was equivalent for patients with and without IBD: 80% [CI 66-89%] and 83% [CI 72-90%], respectively (p = 0.689). All 33 surviving evaluable patients with a history of IBD experienced resolution of IBD by 2 years following allogeneic HCT.
Conclusions: In this cohort, allogeneic HCT was curative for CGD-associated IBD. IBD should not contraindicate HCT, as it does not lead to an increased risk of mortality. This study is registered at clinicaltrials.gov NCT02082353.
Keywords: Allogeneic hematopoietic cell transplantation; allogeneic bone marrow transplantation; allogeneic hematopoietic stem cell transplantation; chronic granulomatous disease; inflammatory bowel disease; primary immunodeficiency.
Conflict of interest statement
Conflict-of-interest disclosure
The authors declare no competing financial interests.
Figures
Similar articles
-
Allogeneic hematopoietic cell transplantation is effective for p47phox chronic granulomatous disease: A Primary Immune Deficiency Treatment Consortium study.J Allergy Clin Immunol. 2024 May;153(5):1423-1431.e2. doi: 10.1016/j.jaci.2024.01.013. Epub 2024 Jan 28. J Allergy Clin Immunol. 2024. PMID: 38290608 Free PMC article.
-
Hematopoietic Cell Transplantation for Chronic Granulomatous Disease in Japan.Front Immunol. 2020 Jul 29;11:1617. doi: 10.3389/fimmu.2020.01617. eCollection 2020. Front Immunol. 2020. PMID: 32849547 Free PMC article.
-
Role of Allogeneic Hematopoietic Stem Cell Transplant for Chronic Granulomatous Disease (CGD): a Report of the United States Immunodeficiency Network.J Clin Immunol. 2019 May;39(4):448-458. doi: 10.1007/s10875-019-00635-2. Epub 2019 May 20. J Clin Immunol. 2019. PMID: 31111420
-
Alloreactivity as therapeutic principle in the treatment of hematologic malignancies. Studies of clinical and immunologic aspects of allogeneic hematopoietic cell transplantation with nonmyeloablative conditioning.Dan Med Bull. 2007 May;54(2):112-39. Dan Med Bull. 2007. PMID: 17521527 Review.
-
Treatment of chronic granulomatous disease with myeloablative conditioning and an unmodified hemopoietic allograft: a survey of the European experience, 1985-2000.Blood. 2002 Dec 15;100(13):4344-50. doi: 10.1182/blood-2002-02-0583. Epub 2002 Aug 8. Blood. 2002. PMID: 12393596 Review.
Cited by
-
Understanding inborn errors of immunity: A lens into the pathophysiology of monogenic inflammatory bowel disease.Front Immunol. 2022 Sep 29;13:1026511. doi: 10.3389/fimmu.2022.1026511. eCollection 2022. Front Immunol. 2022. PMID: 36248828 Free PMC article. Review.
-
Allogeneic bone marrow transplantation for patients with treatment-refractory Crohn's Disease.Heliyon. 2024 Jan 3;10(1):e24026. doi: 10.1016/j.heliyon.2024.e24026. eCollection 2024 Jan 15. Heliyon. 2024. PMID: 38283244 Free PMC article.
-
Chronic Granulomatous Disease (CGD): Commonly Associated Pathogens, Diagnosis and Treatment.Microorganisms. 2023 Sep 5;11(9):2233. doi: 10.3390/microorganisms11092233. Microorganisms. 2023. PMID: 37764077 Free PMC article. Review.
-
Gut Microbiota-Host Interactions in Inborn Errors of Immunity.Int J Mol Sci. 2021 Jan 31;22(3):1416. doi: 10.3390/ijms22031416. Int J Mol Sci. 2021. PMID: 33572538 Free PMC article. Review.
-
Intestinal microbiome and metabolome signatures in patients with chronic granulomatous disease.J Allergy Clin Immunol. 2023 Dec;152(6):1619-1633.e11. doi: 10.1016/j.jaci.2023.07.022. Epub 2023 Sep 1. J Allergy Clin Immunol. 2023. PMID: 37659505 Free PMC article.
References
-
- Marciano BE, Rosenzweig SD, Kleiner DE, et al. Gastrointestinal involvement in chronic granulomatous disease. Pediatrics. 2004;114(2):462–468. - PubMed
-
- Marks DJ, Miyagi K, Rahman FZ, Novelli M, Bloom SL, Segal AW. Inflammatory bowel disease in CGD reproduces the clinicopathological features of Crohn’s disease. Am J Gastroenterol. 2009; 104(1): 117–124. - PubMed
